
Loss of Control on Approach
Colgan Air, Inc.
Operating as Continental Connection Flight 3407
Bombardier DHC-8-400, N200WQ
Clarence Center, New York
February 12, 2009
Accident Report
NTSB/AAR-10/01
PB2010-910401
National
Transportation
Safety Board
NTSB/AAR-10/01
PB2010-910401
Notation 8090A
Adopted February 2, 2010
Aircraft Accident Report
Loss of Control on Approach
Colgan Air, Inc.
Operating as Continental Connection Flight 3407
Bombardier DHC-8-400, N200WQ
Clarence Center, New York
February 12, 2009
National
Transportation
Safety Board
490 L’Enfant Plaza, S.W.
Washington, D.C. 20594

National Transportation Safety Board. 2010. Loss of Control on Approach, Colgan Air, Inc.,
Operating as Continental Connection Flight 3407, Bombardier DHC-8-400, N200WQ, Clarence
Center, New York, February 12, 2009. NTSB/AAR-10/01. Washington, DC.
Abstract: This report discusses the accident involving a Colgan Air, Inc., Bombardier DHC-8-400,
N200WQ, operating as Continental Connection flight 3407, which experienced a loss of control on an
instrument approach to Buffalo-Niagara International Airport, Buffalo, New York, and crashed into a
residence in Clarence Center, New York, about 5 nautical miles northeast of the airport. The safety issues
discussed in this report focus on strategies to prevent flight crew monitoring failures, pilot
professionalism, fatigue, remedial training, pilot training records, airspeed selection procedures, stall
training, Federal Aviation Administration (FAA) oversight, flight operational quality assurance programs,
use of personal portable electronic devices on the flight deck, the FAA’s use of safety alerts for operators
to transmit safety-critical information, and weather information provided to pilots. Safety
recommendations concerning these issues are addressed to the FAA.
The National Transportation Safety Board (NTSB) is an independent federal agency dedicated to promoting
aviation, railroad, highway, marine, pipeline, and hazardous materials safety. Established in 1967, the agency is
mandated by Congress through the Independent Safety Board Act of 1974 to investigate transportation accidents,
determine the probable causes of the accidents, issue safety recommendations, study transportation safety issues, and
evaluate the safety effectiveness of government agencies involved in transportation. The NTSB makes public its
actions and decisions through accident reports, safety studies, special investigation reports, safety recommendations,
and statistical reviews.
Recent publications are available in their entirety on the Internet at <http://www.ntsb.gov>. Other information about
available publications also may be obtained from the website or by contacting:
National Transportation Safety Board
Records Management Division, CIO-40
490 L’Enfant Plaza, SW
Washington, DC 20594
(800) 877-6799 or (202) 314-6551
NTSB publications may be purchased, by individual copy or by subscription, from the National Technical
Information Service. To purchase this publication, order report number PB2010-910401 from:
National Technical Information Service
5285 Port Royal Road
Springfield, Virginia 22161
(800) 553-6847 or (703) 605-6000
The Independent Safety Board Act, as codified at 49 U.S.C. Section 1154(b), precludes the admission into evidence
or use of NTSB reports related to an incident or accident in a civil action for damages resulting from a matter
mentioned in the report.

NTSB Aircraft Accident Report
Contents
Figures .............................................................................................................................................v
Tables ..............................................................................................................................................v
Abbreviations ............................................................................................................................... vi
Executive Summary .......................................................................................................................x
1. .................................................................................................................1Factual Information
1.1 ...................................................................................................................1History of Flight
1.2 ................................................................................................................6Injuries to Persons
1.3 ..............................................................................................................6Damage to Aircraft
1.4 ......................................................................................................................6Other Damage
1.5 ..........................................................................................................6Personnel Information
1.5.1 .................................................................................................................6The Captain
1.5.1.1 ...............................................8Activities in the 72 Hours Preceding the Accident
1.5.1.2
.....................................................................................................9
Federal Aviation Administration Certificate Disapprovals and Colgan Air
Training Events
1.5.2 .......................................................................................................11The First Officer
1.5.2.1 .............................................13Activities in the 72 Hours Preceding the Accident
1.5.2.2 .......................................................................................14Previous Stall Training
1.6. ...........................................................................................................15Aircraft Information
1.6.1 .........................................15Weight and Balance Information and Performance Data
1.6.2 .................................................................................................16Airspeed Indications
1.6.3 .............................................................................................18Stall Protection System
1.6.4 ............................................................................19Ice Detection and Deicing System
1.6.5
................................................................................................21Maintenance Records
1.7 ...............................................................................................22Meteorological Information
1.8 .............................................................................................................23Aids to Navigation
1.9
................................................................................................................24Communications
1.10
............................................................................................................24Airport Information
1.10.1 ....................................................................................................24Air Traffic Control
1.11
.................................................................................................................25Flight Recorders
1.11.1
............................................................................................25Cockpit Voice Recorder
1.11.2 .................................................................................................26Flight Data Recorder
1.12
....................................................................................26Wreckage and Impact Information
1.13 ..............................................................................28Medical and Pathological Information
1.14 .....................................................................................................................................28Fire
1.15
................................................................................................................28Survival Aspects
1.15.1
.........................................................................................28Fire Emergency Response
1.15.2 ............................................................................28Natural Gas Emergency Response
i

NTSB Aircraft Accident Report
1.16 .............................................................................................................30Tests and Research
1.16.1 ......................................................................................30Aircraft Performance Study
1.16.2 ....................................................................31Aircraft Performance Simulation Study
1.17 ...................................................................33Organizational and Management Information
1.17.1 ................................................................................................34Flight Crew Training
1.17.1.1 ......................................................................................................35Stall Training
1.17.1.2 ................................................................................38Winter Operations Training
1.17.1.3 ..............................................................................................39Remedial Training
1.17.1.4 ...............................................................39Crew Resource Management Training
1.17.1.5 ..............................................................................41Captain Leadership Training
1.17.2 ..........................................................................................................42Flight Manuals
1.17.2.1 ........................................................................42Reference and Approach Speeds
1.17.2.2 ...........................................................................42Operations in Icing Conditions
1.17.2.3 ..........................................44Descent, Approach, and Before Landing Checklists
1.17.2.4 ...........................................44Approach Profile and Stabilized Approach Criteria
1.17.3 ........................................................................................45Sterile Cockpit Procedures
1.17.4 ....................................................................................................46Commuting Policy
1.17.4.1 ....................................................47Commuting Status of Pilots Based at Newark
1.17.5 ...........................................................................................................48Fatigue Policy
1.17.6 ....................................................................................................50Crew Room Policy
1.17.7 ........................................................................................................51Safety Programs
1.17.7.1 .........................................................................51Safety Management and Culture
1.17.7.2 ..................................................................................53Safety Reporting Methods
1.17.7.3 .........................................................................54Aviation Safety Action Program
1.17.7.4 .............................................................................55Line Operations Safety Audit
1.17.7.5 ................................................................55Flight Operational Quality Assurance
1.17.7.6 .........................................................................56Additional Postaccident Actions
1.17.7.7 ......................................................57Safety Communications at the Newark Base
1.18 ......................................................................................................57Additional Information
1.18.1 ...........................................................................57Previous Safety Recommendations
1.18.1.1
..................................................................................57Sterile Cockpit Adherence
1.18.1.2 .........................................................................................58Situational Awareness
1.18.1.3
..........................................................................................58Pilot Professionalism
1.18.1.4
.......................................................................59Monitoring Pilot Responsibilities
1.18.1.5 ............................................................................................60Flight Crew Fatigue
1.18.1.6 ......................................................................................................63Stall Training
1.18.1.7
.....................................................65Remedial Training and Additional Oversight
1.18.1.8
.......................................................................................................66Pilot Records
1.18.1.9 ...............................................................................69Air Carrier Safety Programs
1.18.1.10
..........................................................................................70Air Carrier Oversight
1.18.1.11
..........................................................................71Low-Airspeed Alerting System
1.18.1.12
.....................................................................................................72Airplane Icing
1.18.1.13
...........................................................................73Weather Information for Pilots
1.18.2
..............................................................74Federal Aviation Administration Guidance
1.18.2.1 ..........................................................................74Pilot Records Improvement Act
1.18.2.2
............................................................................74Line Operations Safety Audits
ii

NTSB Aircraft Accident Report
1.18.2.3 ................................................................75Flight Operational Quality Assurance
1.18.2.4 ..........................................................................75Standard Operating Procedures
1.18.3
....................................................................................................76
Interview with Colgan Air Flight Crew of Burlington, Vermont
Stick Shaker Event
1.18.4 ........................................................................................77Previous Related Accident
1.18.5 .............................................................78Gulfstream Training Academy Information
2. ...................................................................................................................................80Analysis
2.1 ...............................................................................................................................80General
2.2 .............................................................................................................81Accident Sequence
2.2.1 ...................................................................................................................81Overview
2.2.2 ..................................................................................................83Approach to Airport
2.2.2.1 .........84Possible Reasons for Failed Detection of Impending Stick Shaker Onset
2.2.3 ........................................................................86Response to Stick Shaker Activation
2.2.3.1 .............................................89Possible Reasons for Failed Recovery Procedures
2.2.4 ..............................................................................91Captain’s Management of Flight
2.3 .........................................................................93Strategies to Prevent Monitoring Failures
2.3.1 .............................................................................93Flight Crew Monitoring Training
2.3.2 .............................................................................................95Flight Deck Procedures
2.3.3 ....................................................................................95Low-Airspeed Alert Systems
2.4 .........................................................................................................98Pilot Professionalism
2.4.1 ..................................................................................................98Leadership Training
2.4.2 ...............................................100Sterile Cockpit and Standard Operating Procedures
2.4.3 ..................................................................................103Crew Resource Management
2.5 .............................................................................................................................104Fatigue
2.5.1 ..........................................................106Role of Fatigue in Flight Crew Performance
2.5.2 ........................................................................108Industry Fatigue Mitigation Efforts
2.6 .....................................................................................113First Officer’s Illness Symptoms
2.7 ..............................................................114Captain’s Disapprovals and Training Problems
2.7.1 .........................................................117Remedial Training and Additional Oversight
2.7.2
............................................................................................119Pilot Training Records
2.7.3 ..............................................................................121Pilot Records Improvement Act
2.8 ........................................................................................123Airspeed Selection Procedures
2.9
...................................................................................................................126Stall Training
2.9.1
..............................................................................................128Stick Pusher Training
2.9.2 ...................................................................................................130Simulator Fidelity
2.9.3
..........................................................................................134Tailplane Stall Training
2.10
....................................................................135Federal Aviation Administration Oversight
2.11 ............................................................................................................139Company Policies
2.11.1
....................................................................139Flight Operational Quality Assurance
2.11.2 ...........................142Use of Personal Portable Electronic Devices on the Flight Deck
2.12
..............................................................................................144Safety Alerts for Operators
2.13
....................................................145Preflight Weather Documents and Icing Terminology
2.13.1
.................................................................................145Preflight Weather Documents
2.13.2 ..................................................................................................148Icing Terminology
iii

NTSB Aircraft Accident Report
3. ...........................................................................................................................151Conclusions
3.1
...........................................................................................................................151Findings
3.2
................................................................................................................155Probable Cause
4. ................................................................................................................156Recommendations
4.1
...................................................................................................156New Recommendations
4.2
.....................................159Previously Issued Recommendations Reiterated in This Report
4.3 ..................................160Previously Issued Recommendations Reclassified in This Report
Board Member Statements .......................................................................................................161
5. Appendixes..............................................................................................................................174
Appendix A—Investigation and Hearing ....................................................................................174
Appendix B—Cockpit Voice Recorder Transcript ......................................................................175
iv

NTSB Aircraft Accident Report
Figures
Figure 1. Q400 Indicated Airspeed Display .................................................................................17
Figure 2. Q400 Reference Speeds Switch .....................................................................................18
Figure 3. Q400 Engine Display Showing Ice Detected and Increased
Reference Speeds Message ...........................................................................................20
Tables
Table 1. Injury Chart .......................................................................................................................6
Table 2. Colgan Air’s Approach-to-Stall Training Events ...........................................................35
Table 3. Geographic Distribution of Colgan Air Pilots Based at Newark, New Jersey ...............48
Table 4. Icing Definitions ...........................................................................................................149
v

NTSB Aircraft Accident Report
vi
Abbreviations
AAIB
Air Accidents Investigation Branch of the United Kingdom
AC
advisory circular
ACARS
aircraft communications addressing and reporting system
AFM
airplane flight manual
agl
above ground level
AIM
Aeronautical Information Manual
AIRMET
Airmen’s Meteorological Information
ALB
Albany International Airport
ALPA
Air Line Pilots Association
AOA
angle-of-attack
AOM
airplane operating manual
APM
aircrew program manager
ASAP
aviation safety action program
ASIAS
aviation safety information analysis and sharing
ASOS
automated surface observing system
ASRS
Aviation Safety Reporting System
ATC
air traffic control
ATCT
air traffic control tower
ATIS
automatic terminal information service
ATOS
air transportation oversight system
BTV
Burlington International Airport
BUF
Buffalo-Niagara International Airport

NTSB Aircraft Accident Report
vii
CFM
company flight manual
CFR
Code of Federal Regulations
CRM
crew resource management
CVR
cockpit voice recorder
CWA
Center Weather Advisory
DOD
Department of Defense
eice
en route ice accumulation
EWR
Newark Liberty International Airport
FAA
Federal Aviation Administration
FDR
flight data recorder
FOQA
flight operational quality assurance
FRMS
fatigue risk management system
FSDO
flight standards district office
GIA
Gulfstream International Airlines
Hg
mercury
IAH
George Bush Intercontinental Airport
IAS
indicated airspeed
IATA
International Air Transport Association
ICAO
International Civil Aviation Organization
IEP
internal evaluation program
IFR
instrument flight rules
ILS
instrument landing system
InFO
information for operators
IOE
initial operating experience

NTSB Aircraft Accident Report
viii
LOSA
line operations safety audit
MEM
Memphis International Airport
METAR
meteorological aerodrome report
msl
mean sea level
MSP
Minneapolis-St. Paul International/Wold-Chamberlain Airport
NASA
National Aeronautics and Space Administration
NDB
nondirectional beacon
nm
nautical mile
NOTAM
notice to airmen
NPRM
notice of proposed rulemaking
NTSB
National Transportation Safety Board
NWS
National Weather Service
ORF
Norfolk International Airport
PF
pilot flying
PFD
primary flight display
PIC
pilot-in-command
PIREP
pilot report
PM
pilot monitoring
POI
principal operations inspector
PRIA
Pilot Records Improvement Act
PST
Pacific standard time
QAR
quick access recorder
RDU
Raleigh-Durham International Airport
ROC
Greater Rochester International Airport

NTSB Aircraft Accident Report
ix
SAFO
safety alert for operators
SEA
Seattle-Tacoma International Airport
SIC
second-in-command
SIGMET
Significant Meteorological Information
SMS
safety management system
TSB
Transportation Safety Board of Canada
Vfri
flap retract speed
Vga
go-around speed
V
ref
reference landing speed
VSR
reference stall speed
VMC
visual meteorological conditions
VOR
very high frequency omnidirectional radio range
VVM
verbalize, verify, and monitor
YYZ
Toronto Pearson International Airport

NTSB Aircraft Accident Report
x
Executive Summary
On February 12, 2009, about 2217 eastern standard time, a Colgan Air, Inc., Bombardier
DHC-8-400, N200WQ, operating as Continental Connection flight 3407, was on an instrument
approach to Buffalo-Niagara International Airport, Buffalo, New York, when it crashed into a
residence in Clarence Center, New York, about 5 nautical miles northeast of the airport. The
2 pilots, 2 flight attendants, and 45 passengers aboard the airplane were killed, one person on the
ground was killed, and the airplane was destroyed by impact forces and a postcrash fire. The
flight was operating under the provisions of 14 Code of Federal Regulations Part 121. Night
visual meteorological conditions prevailed at the time of the accident.
The National Transportation Safety Board determines that the probable cause of this
accident was the captain’s inappropriate response to the activation of the stick shaker, which led
to an aerodynamic stall from which the airplane did not recover. Contributing to the accident
were (1) the flight crew’s failure to monitor airspeed in relation to the rising position of the low-
speed cue, (2) the flight crew’s failure to adhere to sterile cockpit procedures, (3) the captain’s
failure to effectively manage the flight, and (4) Colgan Air’s inadequate procedures for airspeed
selection and management during approaches in icing conditions.
The safety issues discussed in this report focus on strategies to prevent flight crew
monitoring failures, pilot professionalism, fatigue, remedial training, pilot training records,
airspeed selection procedures, stall training, Federal Aviation Administration (FAA) oversight,
flight operational quality assurance programs, use of personal portable electronic devices on the
flight deck, the FAA’s use of safety alerts for operators to transmit safety-critical information,
and weather information provided to pilots. Safety recommendations concerning these issues are
addressed to the FAA.

NTSB Aircraft Accident Report
1
1. Factual Information
1.1 History of Flight
On February 12, 2009, about 2217 eastern standard time,
1
a Colgan Air, Inc., Bombardier
DHC-8-400 (Q400),
2
N200WQ, operating as Continental Connection flight 3407,
3
was on an
instrument approach to Buffalo-Niagara International Airport (BUF), Buffalo, New York, when
it crashed into a residence in Clarence Center, New York, about 5 nautical miles (nm) northeast
of the airport. The 2 pilots, 2 flight attendants, and 45 passengers aboard the airplane were killed,
one person on the ground was killed, and the airplane was destroyed by impact forces and a
postcrash fire. The flight was operating under the provisions of 14 Code of Federal Regulations
(CFR) Part 121. Night visual meteorological conditions (VMC) prevailed at the time of the
accident.
The home base of operations for both the captain and the first officer was Liberty
International Airport (EWR), Newark, New Jersey. On February 11, 2009, the captain had
completed a 2-day trip sequence, with the final flight of the trip arriving at EWR at 1544. Also
that day, the first officer began her commute from her home near Seattle, Washington, to EWR
at 1951 Pacific standard time (PST), arriving at EWR (via Memphis International Airport
[MEM], Memphis, Tennessee) on the day of the accident at 0623. The captain and the first
officer were both observed in Colgan’s crew room on February 12 before their scheduled report
time of 1330.
4
The flight crew’s first two scheduled flights of the day, from EWR to Greater
Rochester International Airport (ROC), Rochester, New York, and back, had been canceled
because of high winds at EWR and the resulting ground delays at the airport.
5
The company dispatch release for flight 3407 was issued at 1800 and showed an
estimated departure time of 1910 and an estimated en route time of 53 minutes. The airplane to
be used for flight 3407, N200WQ, arrived at EWR at 1854. A first officer whose flight arrived at
EWR at 1853 saw, as he exited his airplane, the flight 3407 captain and first officer walking
toward the accident airplane. The airplane’s aircraft communications addressing and reporting
system (ACARS) showed a departure clearance request at 1930 and pushback from the gate at
1
All times in this report are eastern standard time based on a 24-hour clock unless otherwise noted.
2
According to Bombardier’s website, the DHC-8 has been known as a Q-series airplane since 1996. The Q400
entered service in 2000.
3
Continental Airlines and Colgan Air were involved in a code-sharing arrangement, but each air carrier had
separate 14 Code of Federal Regulations Part 121 certificates, and Federal Aviation Administration oversight of
each air carrier was conducted by separate certificate management teams.
4
The captain’s and the first officer’s activities before and after their scheduled report time are detailed in
section 1.5.
5
As part of the airlines’ code-sharing arrangement, Colgan flights were subject to cancellation by Continental.
The Colgan EWR regional chief pilot stated, during a postaccident interview, that Continental’s EWR operations
center had called him to cancel multiple Continental Connection flights that day.
NTSB Aircraft Accident Report
2
1945.
6
According to the cockpit voice recorder (CVR) recording, the EWR ground controller
provided taxi instructions for the flight at 2030:28,
7
which the first officer acknowledged.
About 2041:35, the first officer stated, “I’m ready to be in the hotel room,” to which the
captain replied, “I feel bad for you.” She continued, “this is one of those times that if I felt like
this when I was at home there’s no way I would have come all the way out here.”
8
She then
stated, “if I call in sick now I’ve got to put myself in a hotel until I feel better … we’ll see how
… it feels flying. If the pressure’s just too much … I could always call in tomorrow at least I’m
in a hotel on the company’s buck but we’ll see. I’m pretty tough.” The captain responded by
stating that the first officer could try an over-the-counter herbal supplement, drink orange juice,
or take vitamin C.
The CVR recorded the tower controller clearing the airplane for takeoff about 2118:23.
The first officer acknowledged the clearance, and the captain stated, “alright cleared for takeoff
it’s mine.” According to the dispatch release, the intended cruise altitude for the flight was
16,000 feet mean sea level (msl).
9
The flight data recorder (FDR) showed that, during the climb
to altitude, the propeller deice and airframe deice equipment were turned on (the pitot static
deicing equipment had been turned on before takeoff) and the autopilot was engaged.
The airplane reached its cruising altitude of 16,000 feet about 2134:44. The cruise
portion of flight was routine and uneventful. The CVR recorded the captain and the first officer
engaged in an almost continuous conversation throughout that portion of the flight, but these
conversations did not conflict with the sterile cockpit rule, which prohibits nonessential
conversations within the cockpit during critical phases of flight.
10
About 2149:18, the CVR
recorded the captain making a sound similar to a yawn. About 1 minute later, the captain
interrupted his own conversation to point out, to the first officer, traffic that was crossing left to
right. About 2150:42, the first officer reported the winds to be from 250° at 15 knots gusting to
23 knots; afterward, the captain stated that runway 23 would be used for the landing.
About 2153:40, the first officer briefed the airspeeds for landing with the flaps at 15°
(flaps 15) as 118 knots (reference landing speed [V
ref
]) and 114 knots (go-around speed [V
ga
]),
and the captain acknowledged this information. About 2156:26, the first officer stated, “might be
easier on my ears if we start going down sooner.” About 2156:36, the captain instructed the first
officer to “get discretion to twelve [thousand feet].” Less than 1 minute later, a controller from
Cleveland Center cleared the flight to descend to 11,000 feet, and the first officer acknowledged
the clearance.
6
ACARS enables pilots to communicate with company personnel on the ground. ACARS is used to exchange
routine flight status messages and weather information. Some of these messages, such as the time that a flight leaves
the gate, takes off, and touches down, are sent and received automatically.
7
About 7 minutes earlier, the captain had made an announcement over the public address system, indicating
that the taxi delay was the result of the weather conditions at the time.
8
The CVR recorded the first officer sneezing and sniffling.
9
All altitudes in this report are expressed as msl unless otherwise noted.
10
The sterile cockpit rule refers to 14 CFR 121.542, “Flight Crewmember Duties,” which is discussed in
section 1.17.3.

NTSB Aircraft Accident Report
3
About 2203:38, the Cleveland Center controller instructed the flight crew to contact BUF
approach control, and the first officer acknowledged this instruction. The first officer made
initial contact with BUF approach control about 2203:53, stating that the flight was descending
from 12,000 to 11,000 feet with automatic terminal information service (ATIS) information
“romeo,”
11
and the approach controller provided the airport altimeter setting and told the crew to
plan an instrument landing system (ILS) approach to runway 23.
About 2204:16, the captain began the approach briefing. About 2205:01, the approach
controller cleared the flight crew to descend and maintain 6,000 feet, and the first officer
acknowledged the clearance. About 30 seconds later, the captain continued the approach
briefing, during which he repeated the airspeeds for a flaps 15 landing. FDR data showed that the
airplane descended through 10,000 feet about 2206:37. From that point on, the flight crew was
required to observe the sterile cockpit rule.
About 2207:14, the CVR recorded the first officer making a sound similar to a yawn.
About 2208:41 and 2209:12, the approach controller cleared the flight crew to descend and
maintain 5,000 and 4,000 feet, respectively, and the first officer acknowledged the clearances.
Afterward, the captain asked the first officer about her ears, and she indicated that they were
stuffy and popping.
About 2210:23, the first officer asked whether ice had been accumulating on the
windshield, and the captain replied that ice was present on his side of the windshield and asked
whether ice was present on her windshield side. The first officer responded, “lots of ice.” The
captain then stated, “that’s the most I’ve seen—most ice I’ve seen on the leading edges in a long
time. In a while anyway I should say.” About 10 seconds later, the captain and the first officer
began a conversation that was unrelated to their flying duties. During that conversation, the first
officer indicated that she had accumulated more actual flight time in icing conditions on her first
day of initial operating experience (IOE) with Colgan than she had before her employment with
the company.
12
She also stated that, when other company first officers were “complaining” about
not yet having upgraded to captain, she was thinking that she “wouldn’t mind going through a
winter in the northeast before [upgrading] to captain.” The first officer explained that, before
IOE, she had “never seen icing conditions … never deiced … never experienced any of that.”
About 2212:18, the approach controller cleared the flight crew to descend and maintain
2,300 feet, and the first officer acknowledged the clearance. Afterward, the captain and the first
officer performed flight-related duties but also continued the conversation that was unrelated to
their flying duties. About 2212:44, the approach controller cleared the flight crew to turn left
onto a heading of 330°. About 2213:25 and 2213:36, the captain called for the descent and
approach checklists, respectively, which the first officer performed. About 2214:09, the
approach controller cleared the flight crew to turn left onto a heading of 310°, and the autopilot’s
11
An ATIS broadcasts continuous weather observations and other advisory information to pilots operating on
or near an airport. ATIS broadcasts are updated hourly or more frequently if conditions change. ATIS information
“romeo” relayed information from a BUF weather observation at 2154; see section 1.7 for information about the
observation.
12
According to the CVR, the first officer stated, about 2210:58, that she had accumulated 1,600 hours during
flights in the Phoenix, Arizona, area. Section 1.5.2 provides additional details about the first officer’s flying
experience.

NTSB Aircraft Accident Report
4
altitude hold mode became active about 1 second later as the airplane was approaching the
preselected altitude of 2,300 feet. The airplane reached this altitude about 2214:30; the airspeed
was about 180 knots at the time.
About 2215:06, the captain called for the flaps to be moved to the 5° position, and the
CVR recorded a sound similar to flap handle movement. Afterward, the approach controller
cleared the flight crew to turn left onto a heading of 260° and maintain 2,300 feet until
established on the localizer for the ILS approach to runway 23. The first officer acknowledged
the clearance.
The captain began to slow the airplane less than 3 miles from the outer marker to
establish the appropriate airspeed before landing. According to FDR data, the engine power
levers
13
were reduced to about 42° (flight idle was 35°) about 2216:00, and both engines’ torque
values were at minimum thrust about 2216:02. The approach controller then instructed the flight
crew to contact the BUF air traffic control tower (ATCT) controller. The first officer
acknowledged this instruction, which was the last communication between the flight crew and
air traffic control (ATC). Afterward, the CVR recorded sounds similar to landing gear handle
deployment and landing gear movement, and the FDR showed that the propeller condition levers
had been moved forward to their maximum RPM position and that pitch trim
14
in the airplane-
nose-up direction had been applied by the autopilot.
15
About 2216:21, the first officer told the captain that the gear was down; at that time, the
airspeed was about 145 knots. Afterward, FDR data showed that additional pitch trim in the
airplane-nose-up direction had been applied by the autopilot and that an “ice detected” message
appeared on the engine display in the cockpit. About the same time, the captain called for the
flaps to be set to 15° and for the before landing checklist. The CVR then recorded a sound
similar to flap handle movement, and FDR data showed that the flaps had been selected to 10°.
16
FDR data also showed that the airspeed at the time was about 135 knots.
At 2216:27.4, the CVR recorded a sound similar to the stick shaker. (The stick shaker
warns a pilot of an impending wing aerodynamic stall
17
through vibrations on the control
column, providing tactile and aural cues.) The CVR also recorded a sound similar to the
autopilot disconnect horn, which repeated until the end of the recording. FDR data showed that,
13
The pilots set the power lever angle and the propeller condition lever angle for each engine.
14
Pitch trim is used to reduce the long-term pilot or autopilot forces required to maintain a target attitude and
counter the effects of changes to the airplane’s center of gravity, airspeed, or lift during flap extension or retraction.
The pitch trim actuators can be either automatically controlled by the autopilot or manually controlled by a pilot.
For the accident flight, after the autopilot was selected on (shortly after takeoff), the FDR pitch trim adjustments
were applied by the autopilot. (There was no activity in the four discrete parameters dedicated to each pilot’s use of
manual pitch trim once the autopilot was selected on.)
15
FDR data showed the airplane’s airspeed as the following for each of these events: landing gear selected
down, about 180 knots; propeller condition levers selected to maximum, about 170 knots; and pitch trim applied by
the autopilot in the airplane-nose-up direction, about 160 knots.
16
Although the captain called for flaps 15, the flap handle needed to be positioned in the 10° detent before
moving to the 15° detent. The trailing edge flap position reached 10° about 2216:34.
17
Stalls occur when the AOA of the wing—that is, the angle between the direction of airflow and the wing—
exceeds a critical angle at which the air can no longer flow smoothly over the wing. Stalls disrupt lift, increase drag,
and decrease roll control.

NTSB Aircraft Accident Report
5
when the autopilot disengaged, the airplane was at an airspeed of 131 knots. FDR data showed
that the control columns moved aft at 2216:27.8 and that the engine power levers were advanced
to about 70° (rating detent was 80°) 1 second later.
18
The CVR then recorded a sound similar to
increased engine power, and FDR data showed that engine power had increased to about 75
percent torque.
FDR data also showed that, while engine power was increasing, the airplane pitched up;
rolled to the left, reaching a roll angle of 45° left wing down; and then rolled to the right. As the
airplane rolled to the right through wings level, the stick pusher activated (about 2216:34), and
flaps 0 was selected. (The Q400 stick pusher applies an airplane-nose-down control column
input to decrease the wing angle-of-attack [AOA] after an aerodynamic stall.) About 2216:37,
the first officer told the captain that she had put the flaps up. FDR data confirmed that the flaps
had begun to retract by 2216:38; at that time, the airplane’s airspeed was about 100 knots. FDR
data also showed that the roll angle reached 105° right wing down before the airplane began to
roll back to the left and the stick pusher activated a second time (about 2216:40). At the time, the
airplane’s pitch angle was -1°.
About 2216:42, the CVR recorded the captain making a grunting sound. FDR data
showed that the roll angle had reached about 35° left wing down before the airplane began to roll
again to the right. Afterward, the first officer asked whether she should put the landing gear up,
and the captain stated “gear up” and an expletive. The airplane’s pitch and roll angles had
reached about 25° airplane nose down and 100° right wing down, respectively, when the airplane
entered a steep descent. The stick pusher activated a third time (about 2216:50). FDR data
showed that the flaps were fully retracted about 2216:52. About the same time, the CVR
recorded the captain stating, “we’re down,” and a sound of a thump. The airplane impacted a
single-family home (where the ground fatality occurred), and a postcrash fire ensued.
19
The
CVR recording ended about 2216:54.
18
The rating detent for the engine power levers (80° in this case) is a low-force, or soft, detent on the power
quadrant at which the engines’ fully rated power for takeoff, climb, and cruise is achieved. Power lever travel
beyond the rating detent is possible but is available only for emergency use.
19
The postcrash fire was also the result of a severed natural gas service pipeline at the home, as discussed in
section 1.15.2.

NTSB Aircraft Accident Report
6
1.2 Injuries to Persons
Table 1. Injury Chart
Injuries Flight Crew Cabin Crew Passengers Other Total
Fatal
2 2 45 1 50
Serious
0 0 0 0 0
Minor
0 0 0 0 0
None
0 0 0 0 0
Total
2 2 45 1 50
1.3 Damage to Aircraft
The airplane was destroyed by impact forces and a postcrash fire.
1.4 Other Damage
One house and two cars in the driveway of the house were destroyed as a result of the
airplane’s impact and the postcrash fire. The house’s detached garage remained intact, but an
attached garage of an adjacent house was damaged from the impact of a section of the airplane’s
outboard right wing.
1.5 Personnel Information
1.5.1 The Captain
The captain, age 47, held an airline transport pilot certificate and a Federal Aviation
Administration (FAA) first-class medical certificate dated August 22, 2008, with a limitation that
required him to wear corrective lenses while exercising the privileges of this certificate. The
captain received a type rating on the DHC-8 on November 18, 2008.
According to his application for employment with Colgan, from August 2004 to April
2005,
20
the captain attended the first officer program at Gulfstream Training Academy, Fort
Lauderdale, Florida, where he was the second-in-command (SIC) on the Beech BE-1900D for
Gulfstream International Airlines (GIA).
21
Between April and August 2005, the captain worked
20
FAA records indicated that the captain received his private pilot single-engine and instrument certificates in
June 1990 and October 1991, respectively. FAA records also indicated that the captain received his commercial
pilot instrument and single-engine certificates in June 2002 and his multiengine certificate in April 2004.
21
The CVR recorded the captain stating, about 2050:33, “I went through Gulfstream’s program ‘cause … it
was the best program for … the timeframe that I had. You know how fast I wanted to get into the one twenty one
environment … so it really worked out well for me.” Information on the Gulfstream Training Academy is provided
in section 1.18.5.
NTSB Aircraft Accident Report
7
in a non-aviation-related field. He was hired by Colgan in September 2005. The captain reported
on his employment application that, in addition to the BE-1900D, he had flown the Piper PA-32
and PA-28 and the Cessna C-172. He also reported 618 total flight hours, including 38 hours of
actual instrument time, and 71 hours of simulator instrument time.
Colgan’s flight records indicated that the captain had accumulated 3,379 hours of total
flying time, including 3,051 hours in turbine airplanes, 1,030 hours as a pilot-in-command (PIC),
and 111 hours on the Q400. He had flown 116, 56, and 16 hours in the 90, 30, and 7 days,
respectively, before the accident.
22
(These times do not include the accident flight.) The
captain’s transition (from the Saab 340 to the Q400) ground training occurred on October 31,
2008; his transition proficiency check occurred on November 18, 2008; and his transition line
check occurred on December 3, 2008. FAA records indicated that the captain received four
certificate disapprovals (as discussed in section 1.5.1.2). FAA records also indicated no accident
or incident history or enforcement action, and a search of records at the National Driver Register
found no history of driver’s license revocation or suspension.
The check airman who conducted the captain’s Q400 simulator training and line-oriented
flight training characterized the captain’s decision-making abilities as very good. The check
airman stated that the captain, when receiving unusual attitude
23
training in the simulator, had
somewhat overcontrolled the roll axis but had progressed during his subsequent simulator
experience. The check airman who provided the captain with his IOE described the captain’s
performance as good and indicated that his greatest strength was being methodical and
meticulous. Other check airmen indicated that the captain had difficulties with the Q400 flight
management system, but one of the check airmen pointed out that such difficulties were typical
for pilots transitioning to the Q400.
The first officer who flew with the captain on February 10 and 11, 2009, stated that the
captain handled the airplane well, used checklists, and did not miss callouts. The first officer
reported that, during their flights, the captain stated that the workload for the Q400 was
significantly less than that for the Saab 340. First officers who flew with the captain in January
2009 indicated that he flew the Q400 competently. These first officers also indicated that the
captain created a relaxed atmosphere in the cockpit but adhered to the sterile cockpit rule.
The captain’s wife reported that his health was good and that he did not have any injuries
or illnesses in the days before the accident. She also reported that no changes in his health had
occurred in the year preceding the accident. The captain’s wife further reported that the captain
did not take any medications, other than those to treat his hypertension,
24
or nutritional
supplements in the days before the accident and that he drank alcohol occasionally.
22
Colgan could not explain the discrepancy between the captain’s total number of hours on the Q400 (111
hours) and his flight time during the 90 days that preceded the accident (116 hours). There is no record of the
captain flying an airplane other than the Q400 during the 90 days before the accident.
23
Attitude describes an aircraft’s pitch, roll, and yaw in relation to the horizon.
24
According to his wife, the captain was taking Gemfibrozil, Diltiazem, and Hydrochlorot for this purpose.
FAA medical records indicated that the captain had been undergoing treatment for hypertension since 1999, and
these medications were included in his medical records.
NTSB Aircraft Accident Report
8
In addition, the captain’s wife reported that normally he went to sleep about 2200 and
awoke about 0900 or earlier if he were getting up with their children. The captain’s wife
indicated that he would normally receive between 8 and 10 hours of sleep each night and that he
slept well and would sometimes nap. She further indicated that his sleep and wake times when he
worked depended on his schedule.
A first officer who flew with the captain frequently during January 2009 remembered that
the captain had stated that he wanted to get a “crash pad”
25
near EWR but that he was trying to
get around having to pay for a crash pad by bidding trips that had overnights or commutable
ends. This first officer also indicated that the captain had slept in hotels or the EWR crew room
26
during their trips. Another first officer who had flown with the captain in January 2009 indicated
that the captain did not have a crash pad and that he would commute to his home in Florida after
a trip had concluded. According to Colgan, after the accident, the captain’s wife reported that he
did not have a crash pad but that he would sometimes stay overnight with a friend in the EWR
area.
1.5.1.1 Activities in the 72 Hours Preceding the Accident
On February 9, 2009, the captain traveled aboard a commercial air carrier from his home
near Tampa International Airport, Tampa, Florida, to EWR,
27
departing about 1713 and arriving
about 2005.
28
His last known activity on February 9 (a telephone call) ended about 2247. The
first officer who flew with the captain the next day stated that the captain spent the night in the
crew room at EWR. On February 10, the captain began a 2-day trip with a report time of 0530.
The first day of the trip comprised three flights. About 0641, the captain departed EWR and
arrived about 0819 at Toronto Pearson International Airport (YYZ), Toronto, Canada. About
0911, he departed YYZ and arrived about 1049 at EWR. About 1139, the captain departed EWR
and arrived at BUF about 1259. The captain spent the rest of the day at a hotel in the BUF area.
The captain’s duty day on February 10, 2009, was 7 hours 49 minutes, of which 4 hours
36 minutes was flight time. The first officer stated that the airplane encountered icing conditions
briefly while en route to the destination airports. He indicated that the captain engaged the
deicing system and selected the “increase” position for the reference speeds switch
29
before
entering clouds (and disengaged the systems after exiting the clouds). The first officer also
25
This term denotes temporary lodging, such as an apartment or a shared room, used by pilots.
26
The EWR regional chief pilot stated, during a postaccident interview, that the company’s crew room at the
airport has couches, recliners, and a television. The chief pilot described the room as a place for pilots to relax but
indicated that the room was not adequate for rest before a trip. Section 1.17.6 provides additional information about
Colgan’s policy concerning the use of the EWR crew room.
27
The captain had been a commuting pilot since he was hired by the company.
28
The captain’s most recent flight activity before February 9, 2009, began on February 2, when he flew as a
nonrevenue passenger to Albany International Airport (ALB), Albany New York, for a 3-day trip that started the
next day. The trip ended on February 5 at 1522 in ALB; the captain then flew as a nonrevenue passenger to EWR,
arriving at 1742. The captain’s specific activities after that flight are not known (including information about his
return to Tampa), but the captain’s wife described his activities in the days before the accident as routine.
29
The reference speeds switch (commonly referred to as the ref speeds switch) and the deicing system are
discussed in sections 1.6.2 and 1.6.4, respectively.

NTSB Aircraft Accident Report
9
indicated that the captain used the autopilot on approaches and disengaged the autopilot by 800
feet above ground level (agl). The first officer further stated that no extraneous conversations
took place below 10,000 feet (the altitude at which sterile cockpit procedures are in effect).
On February 11, 2009, the captain and the first officer departed the hotel about 0515 to
check in for the second day of their trip, which had a report time of 0615. The second day of the
trip comprised three flights. The captain departed BUF about 0722 and arrived at EWR about
0837. The captain departed EWR about 1003 and arrived at Raleigh-Durham International
Airport (RDU), Raleigh, North Carolina, about 1138. The captain departed RDU about 1334 and
arrived at EWR about 1544.
The captain’s duty day on February 11, 2009, was 9 hours, 49 minutes, of which 5 hours
was flight time. The first officer stated that the captain was well rested and alert during the trip.
The captain’s last known activity that day (logging into the CrewTrac computer system, which
Colgan pilots use to access company-related information, including crew schedules and company
messages) ended about 2151. No information was found regarding where the captain slept that
night.
On February 12, 2009, the captain was scheduled to begin a 3-day trip. At 0310, the
captain logged into the CrewTrac system. While the captain was logged into the system, he
acknowledged a revision to that day’s trip schedule. The captain logged into the CrewTrac
system again at 0726. Two flight crewmembers, who reported at 0655 for a flight that departed
at 0754, saw the captain in the crew room. Another first officer, who reported to EWR at 0525
for a 0632 flight and returned to EWR at 0956, saw the captain asleep in the crew room during
the morning. Between 1012 and 1058, the captain made and received telephone calls. A flight
attendant, who reported to EWR at 1130 for an 1153 flight, stated that she saw the captain eating
lunch.
The EWR regional chief pilot stated that the captain had offered to do office work and
was inserting revisions into airplane manuals between 1200 and 1400.
30
During this time, the
captain made a telephone call to his wife, which lasted a few minutes.
The captain’s specific activities during the remainder of the afternoon are not known, but
he was observed in the crew room watching television and talking with other company pilots. He
logged into the CrewTrac system at 1421 and 1658, made telephone calls at 1624, 1801, 1915,
and 1930,
31
and received a call at 1649.
1.5.1.2 Federal Aviation Administration Certificate Disapprovals and Colgan
Air Training Events
The captain’s record of FAA certificate disapprovals showed the following:
30
The EWR regional chief pilot reported that such administrative duties are considered part of duty time.
31
The call at 1930, to the EWR regional chief pilot’s mobile telephone, lasted 43 seconds.

NTSB Aircraft Accident Report
10
• On October 1, 1991, the captain was disapproved for his instrument airplane rating
during his initial flight check. He flew a PA-28 during the flight test, and the tasks
disapproved were ATC clearance and compliance with ATC clearance, instrument
cockpit check, partial panel32very high frequency omnidirectional radio range
(VOR) approach, nondirectional beacon (NDB) approach, and holding. He passed the
flight test for the rating on October 25, 1991. On his 2005 application for
employment with Colgan,33 the captain stated that he had failed his FAA checkride
for an instrument rating and provided the following explanation: “I missed the NDB
approach, received additional instruction, then repeated the approach and passed.”
• On May 14, 2002, the captain was disapproved for his commercial single-engine land
airplane flight certificate during his initial flight check. He flew a Cessna C-177
during the flight test, and the tasks disapproved were takeoffs, landings, go-arounds,
and performance maneuvers. (He did not report this disapproval on his application for
employment with Colgan.) He passed the flight check for the certificate on June 25,
2002.
• On April 9, 2004, the captain was disapproved for his commercial multiengine land
airplane flight certificate during his initial flight check. He flew a PA-44 during the
flight test and was notified that the entire flight portion of the practical exam would
need to be repeated. (He did not report this disapproval on his application for
employment with Colgan.) He passed the flight check for the certificate on April 29,
2004.
• On October 15, 2007, while a first officer for Colgan, the captain was disapproved for
his airline transport pilot certificate during his initial flight check. He flew a Saab 340
during the flight test, and the disapproved task was approach and landing with a
powerplant failure in a multiengine airplane. He passed the flight check for the
certificate on October 18, 2007.
Colgan’s training records indicated that the captain, while a first officer, needed
additional training in the following areas:
• On October 28, 2005, the captain was graded “train to proficiency” on his initial
proficiency check in the Saab 340. This grade indicated that his overall performance
was satisfactory but that a checkride item (in this case, normal and abnormal
procedures) needed to be repeated during the checkride.
• On October 17, 2006, the captain received an unsatisfactory grade on his recurrent
proficiency check in the Saab 340. The unsatisfactory tasks were rejected takeoffs,
general judgment, landings from a circling approach, oral exam, and nonprecision
approach. The captain attended recurrent training and completed his requalification
proficiency training on November 1, 2006.
32
Partial panel means that certain instruments are covered or are intentionally failed.
33
Colgan’s application for employment asked whether the applicant had “ever failed any proficiency check,
FAA check ride, IOE, or line check.”

NTSB Aircraft Accident Report
11
• On October 3, 2007, the captain received an unsatisfactory grade on his upgrade
proficiency check in the Saab 340. The disapproved task was approach and landing
with a powerplant failure in a multiengine airplane (as stated previously in the FAA
information about this failed flight check). He accomplished upgrade line-oriented
flight training on October 14 and simulator training on October 14 and 15. He
completed a satisfactory upgrade proficiency checkride on October 15, 2007. (These
dates conflict with those in the FAA’s record, which indicated that the captain’s
unsatisfactory checkride occurred on October 15 and his satisfactory checkride
occurred on October 18.)
1.5.2 The First Officer
The first officer, age 24, held a commercial pilot certificate and an FAA first-class
medical certificate dated January 22, 2009, with no limitations. The first officer received a type
rating (SIC privileges only) on the DHC-8 on March 16, 2008.
According to a résumé in her personnel file at Colgan and her application for
employment with the company, from August to December 2006, the first officer worked part
time as a flight instructor at Sawyer Aviation, Scottsdale, Arizona. From January 2007 to
January 2008, the first officer was a flight instructor at Sabena Airline Training Center, Phoenix,
Arizona.
34
She was hired by Colgan in January 2008. Her résumé indicated that she had flown
the following piston-powered airplanes: Piper PA-44, PA-34, and PA-28; Cessna C-152 and C-
172; Beech BE-19 and BE-23; and Diamond DA-40. (The first officer reported no experience
with turbine-powered airplanes on her résumé and employment application.) The first officer had
accumulated 1,470 total flight hours, including 6 hours of actual instrument time, and 86 hours
of simulated instrument time before her employment with Colgan.
Colgan’s flight records indicated that the first officer had accumulated 2,244 hours of
total flying time, including 774 hours in turbine airplanes and on the Q400. She had flown 163,
57, and 16 hours in the 90, 30, and 7 days, respectively, before the accident. (These times do not
include the accident flight.) The first officer’s initial proficiency check occurred on March 16,
2008; her IOE occurred on March 22, 2008; and her recurrent ground school occurred on
January 15, 2009. FAA records indicated that the first officer received a notice of disapproval,
issued on May 7, 2006, for her initial flight instructor certificate. The areas that needed to be
reexamined were technical subject areas; performance maneuvers; preflight procedures; airport
base operations; and takeoff, landings, and go-arounds. (These areas pertained to her
instructional methods and abilities.) She subsequently passed the test and was issued her flight
instructor certificate (airplane single-engine land) on May 12, 2006. FAA records also indicated
no accident or incident history or enforcement action, and a search of records at the National
Driver Register found no history of driver’s license revocation or suspension.
34
The first officer’s résumé and employment application indicated additional aviation-related experience
before her flight instructor positions. She worked as a mechanic’s assistant for Big Bend Aviation, Moses Lake,
Washington, from 2003 (month unknown) to January 2004. Also, she worked at Midstate Aviation, Ellensburg,
Washington, from January 2004 to August 2006, dispatching aircraft, assisting pilots on the Unicom (a common
traffic frequency), and performing office duties.

NTSB Aircraft Accident Report
12
A first officer who went through training with the accident first officer stated that she had
good knowledge of the airplane. The check airman who conducted the first officer’s IOE recalled
that she did not have any problems with handling the airplane and described her as a good pilot
who was sharp, assertive, and thorough. A captain who had flown with the first officer numerous
times indicated that she was average to above average for her level of experience. This captain
further indicated that the first officer, as a monitoring pilot, was always ahead of the airplane and
cross-checked her actions. Other captains indicated that, because of her abilities, the first officer
could have upgraded to captain. None of the captains interviewed after the accident reported any
problems with the first officer’s adherence to sterile cockpit procedures or stated that the first
officer had made any unprompted configuration changes to the airplane while they were the
flying pilot. The ground school instructor for the first officer’s recurrent training stated that she
had good knowledge of the airplane, and another first officer in the class stated that the accident
first officer had more technical knowledge than an average first officer.
In late January 2009, the first officer relocated from Norfolk, Virginia, to the Seattle area
to be closer to family. (She and her husband were living at her parents’ home at the time of the
accident.) She also changed her base from Norfolk International Airport (ORF)
35
to EWR
because it was reportedly easier to commute to EWR from Seattle-Tacoma International Airport
(SEA) than from ORF.
36
The first officer’s husband indicated that she had no significant changes
in her life during the year preceding the accident. He reported that her finances were stable but
that she had taken a significant pay decrease when she began working for Colgan.
37
The first officer’s husband described her as “very healthy” and indicated that she had no
injuries or illnesses in the days before the accident. He acknowledged that she would get sniffles
from cold air but stated that no medication was necessary. The first officer’s husband reported
that she did not take any medications regularly but had taken some ibuprofen 2 days before the
accident after returning home from skiing. He also reported that she drank alcohol occasionally
in social situations.
In addition, the first officer’s husband indicated that she would normally go to sleep
between 2000 and 2200 and awake between 0700 and 1000. Her husband described her sleep
and wake schedule as “very adaptable” and stated that she would sometimes sleep until 1300. He
further stated that she had no difficulties sleeping and no diagnosed sleep disorders.
35
The first officer, while based at ORF, had worked briefly at a coffee shop when not flying. At the time of the
accident, she was not employed outside of Colgan.
36
According to her mother, the first officer had spoken to two other company pilots who lived in the Seattle
area and told her that the commute to EWR was easier from SEA than from ORF because more flights were
available and the distance allowed for sleep opportunities during the flights. The first officer’s mother also stated
that the first officer’s decision to move to the Seattle area was also based on her concern that the ORF base would
close.
37
The CVR recorded the first officer stating, about 2030:02, that she earned a gross salary of $15,800 during
the previous year (her date of hire with the company was January 16, 2008) and that “I’m just lucky ‘cause I have a
husband that’s working.” (The CVR recorded the captain stating that he earned a gross salary of about $60,000
during the previous year.) About 2103:03, the first officer stated that her husband had earned more in one weekend
of military drill exercises than she earned in an entire pay cycle. She added that a recent pay raise would result in an
extra $200 each paycheck.
NTSB Aircraft Accident Report
13
The first officer did not have a crash pad in the EWR area.
38
A captain who had flown
with the first officer when she was based at ORF stated that she planned to stay overnight at
hotels once she began commuting from SEA to EWR.
39
According to a cargo air carrier captain
who met the first officer in December 2008 while they were jumpseat passengers, the first officer
stated that she did not need a crash pad at EWR because she could stay in the crew lounge. A
flight attendant who saw the first officer on the morning of the accident asked her how
commuting was going, to which the first officer replied, “great.”
1.5.2.1 Activities in the 72 Hours Preceding the Accident
On February 8, 2009, the first officer completed a 5-day trip that ended at EWR at 1455.
Specifics of the first officer’s trip from EWR to her home are not known. The first officer’s
husband described her activities in the days preceding the accident as routine. Her telephone
records for February 9 indicate that outbound text messages were sent between 2152 and 2218
PST. According to her husband, the first officer awoke between 0900 and 1000 PST on February
10. Her activities that day included skiing and watching television at home. She went to sleep
between 2000 and 2200 PST.
On February 11, 2009, the first officer awoke between 0900 and 1000 PST. She arrived
at SEA about 1730 PST to board a cargo flight, as a jumpseat passenger,
40
that departed for
MEM about 1951 PST. The captain of this flight spoke with the first officer while the airplane
was being loaded. The captain stated that she seemed to be alert, well rested, and in a good mood
and that she did not show any symptoms of being sick. Another jumpseat passenger (a captain
for the cargo air carrier) reported that the first officer slept for about 90 minutes during the flight.
The flight arrived in MEM about 2330 PST (0230 eastern standard time on February 12).
On February 12, 2009, the first officer traveled from MEM to EWR aboard another cargo
flight that departed about 0418 and arrived about 0623.
41
According to the captain of this flight,
after the airplane landed, the first officer told him that she had slept during the entire flight. The
captain stated that he asked the first officer whether she had a crash pad at EWR and that she
replied that she did not need one. The captain also stated that he asked her what she would be
doing until her report time and that she responded that one of the couches in the crew room “had
her name on it.” In addition, the captain, who met the first officer in December 2008 when both
were jumpseat passengers, stated that she did not appear to be tired and showed no symptoms of
being sick.
38
According to her mother, the first officer was looking into the possibility of getting a crash pad, but she was
concerned about finding appropriate accommodations for a female pilot in a male-dominated profession. The first
officer’s mother also stated that the first officer had planned to bid trips that would allow her to commute.
39
The first officer’s mother stated that the first officer thought it would be less expensive to stay in a hotel
when needed rather than maintain a crash pad.
40
The jumpseat was a normal passenger-type seat located in the cabin of the airplane. The area was free from
interruptions associated with flight deck activities, and no cabin service was provided.
41
The first officer’s mother stated that the first officer had done the same commute before and described it as
easy, stress-free, and less time-consuming than the commute from ORF to EWR.

NTSB Aircraft Accident Report
14
At 0651 the first officer logged into the CrewTrac system and acknowledged changes to
her upcoming trip sequence. At 0732 she made a telephone call to a number associated with
Colgan operations. Two flight crewmembers, who reported at 0655 for a flight that departed at
0754, saw the first officer in the crew room. The first officer’s specific activities on the day of
the accident are not known, but several pilots reported seeing the first officer in the crew room
watching television, talking with other pilots, and sleeping.
42
The first officer also logged into
the CrewTrac system at 1459 and 1625. In addition, telephone records indicated text message
activity during several periods of the day,
43
as well as calls she placed at 1425, 1747, and 1851
and received at 1726.
44
Notable text messages or text message activity included the following:
• At 0729, the first officer sent a text message indicating that she had arrived at EWR
and that her only flight of the day was to BUF. She also indicated that she would be
going to sleep and would call when she woke up.
• At 1305, the first officer sent a text message indicating that she felt good and had
taken a 6-hour nap on a recliner.
• At 1534, the first officer sent a text message referring to her sleep.
• At 2113, during the taxi phase of the accident flight, the first officer sent a text
message.
1.5.2.2 Previous Stall Training
In the year before her employment with Colgan, the first officer was a certified flight
instructor on the Piper PA-28 Archer, which is a light propeller-driven, trainer-type airplane.
According to her supervisor during that time, the first officer had taught or performed between
600 and 1,000 approach-to-stall recoveries. These recoveries would have been performed by the
flying pilot by raising the flaps incrementally during the recovery (at an airspeed that was at least
10 to 15 knots above stall speed) as the airplane accelerated while maintaining altitude. Also,
when she was demonstrating approach-to-stall recoveries to a student, the first officer would
have retracted the flaps herself using her left hand while sitting in the right seat. These
procedures were in contrast with the approach-to-stall training that the first officer received for
the Q400, which was to be performed as a coordinated maneuver with flap changes commanded
by the flying pilot.
45
42
A first officer who reported to EWR at 0525 for a 0632 flight and returned to EWR at 0956 reported seeing
the first officer asleep during the morning. A captain, who had reserve duty at EWR starting at 1400, recalled seeing
the first officer asleep about 1200. Another first officer, who arrived at EWR at 0910 and departed at 1437, reported
seeing the accident first officer asleep in the afternoon. A captain reported that the first officer might have been
asleep during the 1100 to 1400 time period.
43
These periods included the following: 1305 to 1312, 1355, 1416 to 1424, 1514, 1522 to 1534, 1611 to 1612,
1635 to 1636, 1646 to 1647, 1659, 1723, and 1958. The first officer’s husband stated that he and the first officer
had sent text messages throughout the morning (PST) and that he had awakened her from a nap with a text message
or a telephone call that he initiated.
44
The husband of the first officer indicated that he spoke with her sometime between 1400 and 1500 and that
she sounded “great” during the conversation.
45
Colgan’s approach-to-stall training is discussed in section 1.17.1.1.

NTSB Aircraft Accident Report
15
1.6. Aircraft Information
The Q400 is manufactured by Bombardier, Inc., as a medium-range, all metal, high-wing,
T-tail airplane powered by two turbopropellers. The airplane was certified for flight in icing
conditions according to the requirements of 14 CFR Part 25 Appendix C and was designed to
carry 74 passengers and 4 crewmembers. The accident airplane was manufactured in April 2008.
The airplane was equipped with two Pratt & Whitney Canada PW150A engines and two Dowty
R408/6-123-F17 six-bladed propellers. At the time of the accident, the airplane had accumulated
1,819 total hours and 1,809 total flight cycles. (A flight cycle is one complete takeoff and
landing sequence).
1.6.1 Weight and Balance Information and Performance Data
Colgan was authorized by the FAA to contract with AeroData, Inc., for weight and
balance information and real-time takeoff, en route, and landing performance data for its Q400
airplanes. (AeroData’s information was derived from the Bombardier Q400 Airplane Flight
Manual [AFM].) Flight crews were to request these performance data using ACARS.
The Colgan Q400 company flight manual (CFM) explained how flight crews were to
transmit a landing data request and receive landing performance data from AeroData.
Specifically, crews were required to enter the airport, runway, and airplane gross landing weight
and could enter a secondary runway, flap setting, and wind.
46
This information was transmitted
via datalink to the AeroData computer system, which would provide the required performance
data on the ACARS display within 10 to 30 seconds. These data included V
ref
(reference landing
speed), V
ga
(go-around speed), the flap retract speed (V
fri
), the climb speed, and the maximum
allowable landing weight and landing distance. The AeroData system provided the accident
flight crew with landing performance information, including a V
ref
of 118 knots, at 2153.
A Colgan check airman explained that, in the remarks section of the data request screen,
flight crews could enter the keyword “icing,” which would cause the V
ref
speed provided by the
AeroData computer system to increase by 20 knots for a flaps 15 landing and 15 knots for a flaps
35 landing. The check airman also stated that crews could enter the keyword “eice” (en route ice
accumulation), which would add 90 pounds to the airplane’s calculated landing weight to
compensate for the accumulated ice. The accident flight crew did not enter the keywords “icing”
or “eice” in its request to AeroData. (AeroData provided the downlink from the accident
airplane, and the area in which the keywords “icing” and “eice” would have appeared if they had
been entered was blank.) If the flight crew had made either entry, then AeroData would have
provided a V
ref
of 138 knots to the crew.
On November 23, 2009, Colgan issued Flight Standards Memo 09-013 regarding
AeroData keyword inputs. The memo stated that, if keywords such as “icing” or “eice” were
misspelled, AeroData would provide the clean (no ice) landing speeds. The memo indicated that,
46
If a flap setting or wind was not entered, then the AeroData system would provide an optimal flap setting and
assume that the winds were calm.

NTSB Aircraft Accident Report
16
for any previous AeroData requests that included a misspelling of these words, the discrepancy
could have been noticed in the remarks section of the landing report returned by AeroData,
which would have shown “none” instead of “icing conditions.” The memo further stated that
AeroData has corrected this issue so that any misspelled keywords would result in the error
message, “invalid keyword,” and include the keyword that is not recognized.
1.6.2 Airspeed Indications
Airspeed indications on the Q400 are located on the left and right primary flight displays
(PFD). According to the Q400 Airplane Operating Manual (AOM), indicated airspeed (IAS) is
displayed digitally on the vertical scale (or airspeed tape) on the left side of the PFD. The
vertical scale shows the airplane’s current IAS with marks every 10 knots to ± 42 knots from the
actual IAS. The airspeeds that could be displayed on the vertical scale ranged from 30 to 500
knots. An airspeed trend vector (an upward- or downward-facing white arrow) indicates whether
the airspeed is increasing or decreasing. According to Bombardier, the airspeed trend vector
predicts the airspeed at which the airplane will be flying in 10 seconds. Five “bugs” indicate the
airspeeds that may be programmed by the flight crew for takeoff, and two bugs indicate the
airspeeds that may be programmed for landing. The two bugs that can be displayed for landing
are represented on the airspeed indicator by a solid blue triangle and an open blue triangle, which
Colgan used for V
ref
and V
ga
, respectively.
A low-speed cue is shown as a red and black vertical bar that extends from the bottom
right of the vertical scale. The low-speed cue warns pilots of an inappropriately low airspeed for
the airplane configuration or operating condition.
47
If the airplane’s IAS is less than or equal to
the IAS at the top of the low-speed cue, the stick shaker activates. Also, the numbers on the IAS
display change from white to red, providing pilots with another visual warning of an
inappropriately low airspeed. Figure 1 shows the IAS digital display on the Q400 PFD.
47
The low-speed cue can also represent the minimum control speed during approach and landing with all
engines operating.
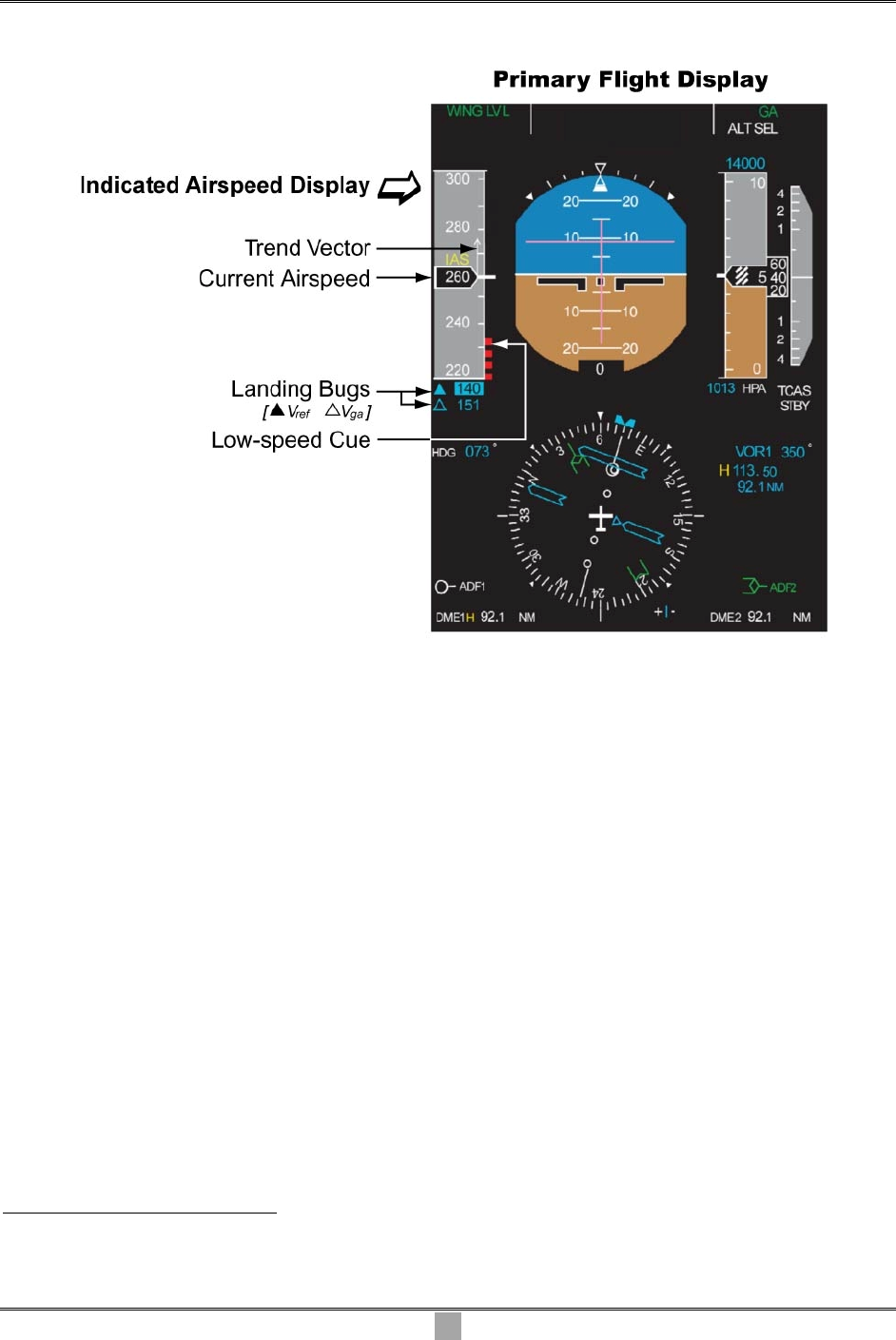
NTSB Aircraft Accident Report
17
Figure 1. Q400 Indicated Airspeed Display
Source: Bombardier.
The ice protection panel, which is located on the overhead panel on the captain’s side of
the cockpit, includes a “REF SPEEDS” switch that can be set to the INCR (increase) or OFF
positions, as shown in figure 2. During the May 2009 public hearing on this accident,
48
an
engineering manager from Bombardier stated that the ref speeds switch, when set to the increase
position, advances the stall warning so that the stick shaker would activate at a lower AOA;
49
as
a result, the airplane would have the same performance margins relative to the stall speed during
operations in icing conditions as it would have with a clean (no ice accretion) configuration (and
the ref speeds switch set to the off position). The engineering manager also stated that, because
the stick shaker would activate at a lower AOA with the ref speeds switch set to the increase
position, the flight crew would need to increase landing airspeeds between 15 and 25 knots
depending on the flap setting (to remain above the stall warning threshold).
48
Appendix A provides information about the public hearing for this accident.
49
The ref speeds switch position does not change the AOA value that triggers stick pusher activation.

NTSB Aircraft Accident Report
Figure 2. Q400 Reference Speeds Switch
Source: Bombardier.
The Bombardier Q400 AFM, section 4.7.2, Ice Protection Procedures, dated July 13,
2005, stated that the ref speeds switch was to be in the increase position before entering icing
conditions and in the off position after the airplane is aerodynamically clean (that is, all ice is
removed from the visible leading edges and wing tips). The Q400 AFM also cautioned that a
stall warning might occur if airspeed was not increased before the ref speeds switch was selected
to the increase position. The ref speeds switch on the accident airplane was found in the increase
position.
1.6.3 Stall Protection System
The Q400 stall protection system includes a stick shaker and stick pusher. The stick
shaker is a stall warning device on each control column that provides pilots with an aural and
tactile warning of an impending stall. Even though the stick shaker on each control column is
independently controlled by one of two units in the stall protection system, both columns vibrate
simultaneously when a stick shaker activates because both columns are interconnected.
18
NTSB Aircraft Accident Report
19
The Q400 stick pusher is a stall identification device that, according to Bombardier,
positions the elevator to 2° nose down and provides a nose-down input to both control columns
after an AOA threshold has been reached and an aerodynamic stall has occurred.
50
The stick
pusher thus provides pilots with a tactile cue that they need to push forward on the control
column to gain airspeed and alleviate the stall condition rather than pull back on the column. The
stick pusher was designed to remain engaged (subject to certain constraints)
51
until the AOA
decreases below the stick shaker activation angle. The engineering manager from Bombardier
testified at the public hearing that the stick pusher system could be overpowered or disengaged
by flight crew action.
52
The airplane’s two stall protection modules provide output commands to the stick shaker
and stick pusher. The stall protection modules use AOA, flap position, body axis attitudes,
normal acceleration, true airspeed, Mach number,
53
engine torque, and icing status data to
calculate when the airplane is approaching a stall condition. The stick shaker activates when
these parameters, in particular AOA, reach a specific threshold. The Q400 AOM stated that,
when the stall protection modules operate the stick shakers, the autopilot automatically
disengages,
54
and the ground proximity warning system “pull up” alert is inhibited. In addition,
the stall protection modules use AOA, flap position, body axis attitudes, normal acceleration,
true airspeed, Mach number, power lever angle, and condition lever angle data to calculate the
AOA at which the stick pusher activates.
1.6.4 Ice Detection and Deicing System
At the public hearing, an engineering manager from Bombardier testified that visual cues
provide the most reliable means of ice detection.
55
In addition, ice detector probes are installed
on each side of the Q400 forward fuselage, below the pilot’s and copilot’s windows, to detect
when ice is accumulating on the airplane. When ice accumulates on the probe sensors, the probes
send an electronic signal to the avionics system to indicate that ice is present. The ice detector
probes also cycle heat to the sensors to melt ice and ensure that the sensors can continue
50
It is important to note that the Q400 stick pusher system differs from the stick pusher systems on other
regional airplanes (for example, the CRJ-200 and ATR-42/72), which activate before a stall occurs. These stick
pusher systems were designed to warn pilots of, and prevent them from encountering, undesirable pre-stall and stall
characteristics.
51
These constraints include limits on radio altitude, bank angle, pitch attitude, and normal load factor.
52
The Bombardier engineering manager further testified that the nominal control column force was significant
enough to get a pilot’s attention to relax back pressure on the column but was not too excessive for a pilot to
override if an inadvertent system failure had occurred. Overriding the stick pusher requires 80 pounds of opposite
breakout force and then 66 pounds of sustained force. Disengaging the pusher is accomplished by pressing the stick
pusher shutoff switchlight on the glareshield.
53
Mach number equals an object’s speed divided by the speed of sound.
54
The airplane’s autopilot can also be disengaged manually. An autopilot button is located on the automatic
flight control system control panel, which is mounted on the glareshield directly in front of a flight crew. An
autopilot disengage button is also located on each control wheel.
55
According to Bombardier, observations of the outboard wing leading edge and the windshield wiper spigots
are the primary means to indicate when an airplane has entered icing conditions. During nighttime operations, the
spigots can be illuminated by a lamp inside the cockpit.

NTSB Aircraft Accident Report
20
detecting ice. The ice detection probe sensors have a continuous self-testing feature to ensure
that they are working properly. When both sensors fail, an “ice detect fail” light illuminates on
the caution and warning panel in the cockpit.
56
The Q400 engine display shows an “ICE DETECTED” message, as shown in figure 3,
when one or both ice detector probes detect more than 0.5 millimeter (0.02 inch) of ice. The
message appears in reverse video (black letters on a white background) for 5 seconds if the ref
speeds switch has already been set to the increase position. After the 5-second period, the
message appears in normal video (white letters on a black background, as shown in figure 3)
when ice is detected and the ref speeds switch remains set to the increase position. If the ref
speeds switch is set to the off position when ice is detected, the message flashes with yellow
letters on a black background until the switch is turned to the increase position. In addition,
when the switch has been selected to the increase position, an “INCR REF SPEED” message
(also shown in figure 3) appears in normal video, regardless of whether ice has been detected.
Figure 3. Q400 Engine Display Showing Ice Detected and Increased Reference
Speeds Message
Source: Bombardier.
The ice detected message appears periodically during icing conditions—the message is in
view for a minimum of 60 ± 5 seconds when ice is detected—and is out of view when no ice is
56
The CVR did not record the crew discussing the illumination of this or any other caution light.

NTSB Aircraft Accident Report
21
detected. For the accident flight, FDR data showed that the ice detected parameter transitioned
from “not detected” to “detected” and then transitioned back to “not detected” during the
following times: 2207:53 to 2208:53, 2209:21 to 2211:05, and 2211:17 to 2212:17. FDR data
also showed that the parameter transitioned from “not detected” to “detected” from 2216:25 to
the end of the recording.
57
The airplane’s airframe deicing system uses bleed air from the engines to inflate rubber
boots that break apart accumulated ice on the wing and tail (horizontal stabilizer and vertical
stabilizer) leading edges as well as the nacelle air intakes.
58
The propeller deicing system
includes electrical heating elements in the leading edge of each propeller blade to remove ice
accumulations. A rotary switch on the ice protection panel is used to select propeller heat. Both
front windshields and the pilot’s side window have electronically controlled heater elements that
are laminated into the panels. These heater elements are designed to keep the windshield and
windows at a predetermined temperature to prevent icing and misting.
1.6.5 Maintenance Records
Two line checks were performed on the accident airplane on the day of the accident after
the airplane had arrived at Albany International Airport (ALB), Albany, New York, from
EWR.
59
The ice detector probes and deice boots were checked visually, with no discrepancies
reported.
Also, the flight crew of the flight from EWR to ALB reported, in the airplane’s logbook,
that an “ice detect fail” caution light had illuminated during the flight. Maintenance personnel at
ALB replaced the right-side ice detector probe and reported that an operational check of the ice
detection system was satisfactory.
A review of the accident airplane’s logbook from April 2008 to February 2009 revealed
no chronic issues with the airplane’s primary or secondary flight control systems. Also, no
discrepancies with the primary or secondary flight control systems were reported after the
airplane’s last L-1, L-2, and A checks.
60
57
The FDR showed that the airplane was at the following altitudes when the ice detected parameter
transitioned from “not detected” to “detected”: about 8,700 feet, about 7,300 feet, about 5,300 feet, and about 2,400
feet.
58
The ice protection panel, shown in figure 2, includes a total of 14 boot inflation advisory lights that allow
pilots to monitor deicing boot operation. Pilots can also check the operation of the wing deice boots by looking out
their windows at the boots.
59
Line checks involve servicing and a walk-around visual inspection of the airplane’s general condition. The
first line check, known as the L-1 check, is accomplished every 3 days or 36 flight hours, whichever occurs first.
The second line check, known as the L-2 check, is performed every 6 days or 50 flight hours, whichever occurs
first.
60
A checks are performed every 400 flight hours. The accident airplane’s last A and 2A checks were
performed on December 24, 2008, and the last 3A check was performed on October 23, 2008.

NTSB Aircraft Accident Report
22
1.7 Meteorological Information
BUF has an automated surface observing system (ASOS) that is maintained by the
National Weather Service (NWS). The FAA is responsible for the augmentation and backup of
the ASOS, which are provided by NWS-certified observers at BUF. The ASOS records
continuous information on wind speed and direction, cloud cover, temperature, precipitation, and
visibility in statute miles. The ASOS transmits an official meteorological aerodrome report
(METAR) each hour and special weather observations as conditions change. The ASOS also
records weather observations every 5 minutes, but this information is not disseminated to pilots.
The 2154 METAR for BUF indicated winds from 240° at 15 knots gusting to 22 knots,
visibility 3 miles in light snow and mist, a few clouds at 1,100 feet agl, ceiling broken at 2,100
feet agl, overcast at 2,700 feet agl, temperature 1° C, dew point -1° C, and altimeter 29.79 inches
of mercury (Hg). (This METAR became the basis for ATIS information “romeo.”) The 5-minute
observation at 2215 indicated wind from 250° at 14 knots, visibility 3 miles in light snow and
mist, a few clouds at 1,100 feet agl, ceiling overcast at 2,100 feet agl, temperature 1° C, dew
point -1° C, and altimeter 29.80 inches of Hg.
The NWS terminal aerodrome forecast that was current at the time of the accident was an
amended forecast issued at 1920. The amended forecast expected, from 1900 to 2100, winds
from 240° at 15 knots, visibility 1 1/2 miles in light snow showers, and ceiling overcast at 1,500
feet agl. From 2100 to 0100, the forecast expected winds from 250° at 14 knots gusting to
24 knots, visibility 5 miles in light snow showers and mist, and ceiling overcast at 2,000 feet agl.
Numerous pilot reports (PIREPs) about icing conditions in the BUF area were received
during the day of the accident between 1250 and 1815. These PIREPs included reports of light,
light-to-moderate, and moderate rime icing from 3,000 to 14,000 feet in the BUF area.
61
The
1815 PIREP, which was received from an Airbus A319 pilot about 4 hours before the accident,
reported light-to-moderate rime icing at 5,000 feet and a temperature of -7° C.
The weather document for the accident flight (which accompanied the dispatch release)
did not include pertinent NWS Airmen’s Meteorological Information advisories (AIRMETs),
62
which inform pilots of significant weather phenomena. One of these AIRMETs extended over
the airplane’s route and expected moderate rime icing from below 8,000 feet. Another AIRMET
extended over a larger region in the northeast, including the accident site, and expected
occasional moderate icing below 18,000 feet. The icing conditions in both AIRMETs were
expected to continue from 2145 to 0400 the next day. Other AIRMETs were in effect for
instrument flight rules (IFR) conditions and turbulence over the BUF area. The only icing
information included in the weather document consisted of the reports and forecast of snow at
61
The FAA’s Aeronautical Information Manual, chapter 7, Safety of Flight, section 7-1-21, describes rime ice
as rough, milky, opaque ice formed by the instantaneous freezing of small supercooled water droplets.
62
An AIRMET is one of five weather advisory categories used by the NWS. The other categories are Severe
Weather Forecast Alerts, Significant Meteorological Information (SIGMETs), Convective SIGMETs, and Center
Weather Advisories (CWAs). AIRMETs, SIGMETs, and Convective SIGMETs are issued from the NWS Aviation
Weather Center in Kansas City, Missouri, and CWAs are issued from NWS Center Weather Service Units within
FAA centers.

NTSB Aircraft Accident Report
BUF and two PIREPs indicating light-to-moderate rime icing in the BUF area between 3,000 and
14,000 feet.
The ATC transcript showed that, after the accident, the controller who was handling the
accident flight asked pilots of other airplanes whether icing was occurring. About 2221:12, a
Delta Air Lines pilot, whose airplane was at an altitude of 2,300 feet at the time, told the
controller that the airplane was not accumulating any ice at that altitude but that some ice might
have been accumulating while descending between 6,500 and 3,500 feet. About 2225:11, the
pilot reported that the airplane had accumulated between 1/4 and 1/2 inch of ice during the
descent. About 2225:25, a US Airways pilot reported that his airplane, which was south of the
airport and had been cleared to descend from 5,000 to 2,300 feet, had been accumulating rime
ice for about 10 minutes. The controller asked the pilot to let him know when the airplane was
out of icing conditions and mentioned that pilots of other arriving airplanes that were south of
the airport did not report similar icing conditions. About 2227:04, after being instructed to
maintain 2,300 feet until established on the localizer, the pilot reported that ice was starting to
come off the windscreen.
The National Transportation Safety Board (NTSB) conducted a postaccident survey of
pilots operating into BUF about the time of the accident to determine the icing environment at
the time. Of the 22 surveys issued, 12 (about 55 percent) were returned. The survey found that
varying (trace, light-to-moderate, and moderate) intensities of icing conditions were occurring
between 2,000 and 12,000 feet. The surveys indicated that the pilots were aware of the potential
for icing conditions and were not surprised by the encounters. None of the pilots indicated that
they had formally reported the icing conditions because the pilots did not consider the icing
conditions to be significant.
Ten of the surveys were from pilots of air carrier jet airplanes; two of the surveys were
from pilots of turboprop airplanes. The two turboprop airplanes were an AirNow Embraer EMB-
110 and another Colgan Q400 (flight 3268, also from EWR to BUF), which landed about 2200
and 2230, respectively. The AirNow pilot reported moderate rime ice while descending between
5,000 and 2,000 feet, with 2 to 3 inches of ice accumulation noted on the propeller spinners and
some unprotected areas after arriving at BUF. The AirNow pilot also stated that the flight was in
icing conditions for about 10 minutes. The Colgan Q400 pilot reported light-to-moderate rime
ice while descending between 5,000 and 3,000 feet.
1.8 Aids to Navigation
During a postaccident interview, one air carrier reported that, when some of its airplanes
attempted to intercept the BUF runway 23 ILS from a right downwind position, the glideslope
would indicate that the airplane was well above the glideslope. The air carrier further reported
that, just before intercepting the localizer, the glideslope would move upward to the proper
interception indication. As a result, airplanes that had the autopilot and flight director engaged
23

NTSB Aircraft Accident Report
24
would capture the glideslope as it moved up, which would result in a climb and loss of
airspeed.
63
The accident flight intercepted the ILS from the left side,
64
and no problems with this or
any other navigational aid was reported for flight 3407.
1.9 Communications
No technical communications problems were reported.
1.10 Airport Information
BUF is located 5 miles east of Buffalo, New York, at an elevation of 728 feet. BUF has
two runways, 5/23 and 14/32; runways 5/23 and 32 had published ILS instrument approach
procedures. The ILS runway 23 approach plate, dated April 20, 2007, included a note stating,
“glideslope unusable beyond 5° right of course.”
1.10.1 Air Traffic Control
BUF is a combined ATCT and terminal radar approach control. Radar data are provided
by an airport surveillance radar-9 at the airport.
The accident flight was handled by the BUF approach controller at the east radar
position. The controller stated that, after he instructed the flight crew to contact the ATCT, he
continued to monitor the airplane’s progress. The controller reported seeing the altitude readout
in the radar display data block change to “XXX,” which was an indication that the radar system
had interpreted the altitude readout to be unreliable. Afterward, the airplane target and the data
block disappeared from the radar display.
The approach controller contacted the tower controller to find out if something had
happened to the flight and asked the tower controller to attempt to contact the airplane. The ATC
transcript showed that both controllers attempted to contact the airplane during the next minute.
The approach controller also asked the pilot of a Delta Air Lines airplane (which was being
vectored for an ILS approach to runway 23) to see if the Colgan airplane was off to the right.
The pilot of the Delta flight reported that he did not see the airplane and that no target for it
appeared on the traffic alert and collision avoidance system. The approach controller reported
that this information seemed to be confirmation that the airplane had been involved in an
63
The National Aeronautics and Space Administration’s Aviation Safety Reporting System (described in
section 1.17.7.3) received several reports regarding the BUF glideslope issue, including one report dated December
2004, two reports dated January 2009, and one report dated April 2009.
64
The FDR showed that the airplane had not captured the glideslope.

NTSB Aircraft Accident Report
25
accident. The controller asked the controller-in-charge to call the airport fire department, which
coordinated all off-airport events.
The approach controller who handled the accident flight stated that he then began trying
to figure out what had happened to the flight. He asked other airplanes operating in the area
about icing (as previously indicated in section 1.7) and learned that some airplanes had
encountered icing but that the conditions did not seem to be “especially serious.” The controller
also checked the ILS monitor panel to see if a problem had occurred with the ILS equipment but
found everything working normally. The controller was notified that an accident had occurred by
the controller-in-charge, who had been told of the accident by the airport fire department about
10 minutes after the loss of contact with the flight.
The controller stated that icing conditions were common in the BUF area throughout
most of the winter and characterized the icing conditions on the day of the accident as “routine
stuff that pilots fly in here every day.” Also, he indicated that the air traffic at the time of the
accident was “fairly typical.”
1.11 Flight Recorders
1.11.1 Cockpit Voice Recorder
The airplane was equipped with a Honeywell model 6022 SSCVR 120 solid-state CVR,
serial number 97896. The CVR did not sustain any heat or structural damage. The audio
information was extracted normally and without difficulty.
The CVR was sent to the NTSB’s laboratory for readout. The CVR recording contained a
2-hour 1-minute digital recording of a flight crew microphone channel and a cockpit area
microphone channel. Both channels contained excellent-quality audio data.
65
Also, for the last
30 minutes of flight, the CVR contained four channels
66
of excellent-quality audio data. (The
last 30 minutes of the two 2-hour channels recorded the same information as the four 30-minute
channels.) A transcript was prepared of the recording (see appendix B).
A CVR sound spectrum study was performed to resolve an inconsistency involving stick
shaker activation information. Specifically, the CVR transcript indicated the stick shaker was
only audible from 2216:27.4 to 2216:34.1 and from 2216:35.4 to the end of the recording
(2216:53.9). During the 1.3-second time period during which the stick shaker was not audible on
65
The NTSB rates the audio quality of CVR recordings according to a five-category scale: excellent, good,
fair, poor, and unusable. The NTSB considers an excellent-quality audio recording to be characterized by the
following traits: virtually all of the crew conversations could be accurately and easily understood. The transcript that
was developed might indicate only one or two words that were not intelligible. Any loss in the transcript was
usually attributed to simultaneous cockpit/radio transmissions that obscured each other.
66
The first through fourth channels were the passenger address system, the captain’s station, the first officer’s
station, and the cockpit area microphone, respectively.
NTSB Aircraft Accident Report
26
the CVR, an FDR sample (at 2216:34.6) indicated that the stick shaker was active.
67
The sound
spectrum study revealed evidence of stick shaker operation between 2216:34.4 and 2216:35.4,
but the study did not identify any frequency content consistent with stick shaker activation
between 2216:34.1 and 2216:34.4.
1.11.2 Flight Data Recorder
The airplane was equipped with a Honeywell model 980-4700 FDR, serial
number 14241. The FDR recorded flight information in a digital format using solid-state
memory as the recording medium. Of the total number of parameters recorded by the FDR, 121
parameters were deemed to be relevant to the circumstances of the accident.
68
The FDR was sent to the NTSB’s laboratory for readout and evaluation. The FDR was in
good condition, and the data were extracted normally. About 26 hours 30 minutes of data were
recorded on the FDR, including about 58 minutes of data from the accident flight. The FDR
recording ended about 2216:53.
1.12 Wreckage and Impact Information
The airplane wreckage was mostly contained within the property boundaries at 6038
Long Street, Clarence Center, New York.
69
The airplane was severely fragmented with extensive
fire damage. About 60 percent of the main structural components could be conclusively
identified, including structure from the radome and both wingtips. The empennage was found
intact in the wreckage. Numerous small pieces of airplane structure were recovered but were not
conclusively identified. The airplane wreckage was on a magnetic heading of 070°. All of the
examined fracture surfaces exhibited signs that were consistent with overload failure; no
evidence indicated any preimpact failures
. Flight control continuity could not be determined
because of severe fragmentation and burn damage.
The airplane impacted the south side of the house near ground level, and pieces of the
airplane traveled through the house, coming to rest beyond the northeast corner of the house’s
foundation. A ground scar, which was found on the south side of the house about 10 feet south of
the south foundation wall, measured 15 feet long, 5 feet wide, and 3 feet deep. Two trees along
the southern boundary of the property were impacted by the airplane and had their tops sheared
off. One tree strike occurred about 20 feet agl, and the other occurred about 25 feet agl. Tree
67
The FDR recorded the activation of the stick shaker at 2216:30.6.
68
Title 14 CFR 121.343, “Flight Data Recorders,” required the airplane to be equipped with an FDR that
recorded a minimum of 88 parameters.
69
As discussed in section 1.4, a section of the outboard leading edge of the right wing impacted the garage of
an adjacent house located to the south of the destroyed house. Also, the right forward cargo door was recovered
across the street from, and east of, the destroyed house with impact damage but little fire damage. In addition, the
only structure found after a search of the rooftops and yards that surrounded the destroyed house was a small
section of propeller spinner.

NTSB Aircraft Accident Report
27
debris located between the property boundary and the house exhibited clean, angled cuts that
were consistent with propeller impact.
The right main landing gear exhibited minor fire damage to the tires, the retract actuator
was broken off in the almost fully retracted position, and the right main landing gear uplock (a
mechanical lock to hold the gear in the up position) was found in the open position. The left
main landing gear exhibited severe fire damage with the retract actuator broken off in the almost
fully retracted position, but the left main landing gear uplock was not conclusively identified.
The nose landing gear was found with severe fire damage, but no conclusive evidence of the
gear’s position was found.
The stage 1 low pressure compressors in both engines were found with blades bent in the
direction opposite rotation, fractured blades, airfoil leading edge impact damage, and ingested
dirt. No evidence of a turbine failure or an uncontainment was found in either engine. Both
engine power levers and the No. 1 engine condition lever appeared to be in the full forward
position, and the No. 2 engine condition lever appeared to be in its midrange position. Parts of
each blade tip from both propellers were found. Six No. 1 propeller blades and four of six No. 2
propeller blades were found almost full length and were fractured near the root of the blades
(where the blades are installed into the propeller hub).
The ice protection panel was recovered in the wreckage and was found to be severely
burned. As indicated in section 1.6.2, the ref speeds switch was found set to the increase
position. The ice detector probes were not identified in the wreckage.
No segments of the leading edge deice boots from the left wing were identified. Two
leading edge sections from the right wing were located in the wreckage. The deice boots from
these sections appeared to still be bonded to the leading edge, except in some areas that appeared
to be associated with impact damage. The pneumatic lines leading to the connections on the
inside of the leading edge sections were intact. These and other deice system pneumatic lines did
not show any evidence of leaks, ruptures, or missing or damaged line couplings.
70
The leading
edge deice boots for the horizontal and vertical stabilizer were found in good condition. The
boots were still bonded to the leading edge structure, with only minor tears in the boot surfaces
and slight charring on the left horizontal stabilizer boot.
Portions of all eight flap actuators (which move the flap surfaces to a selected position
and maintain the selected position against the aerodynamic forces acting on the flap surfaces)
were recovered. Seven of the actuators contained the appropriate portions to measure the
dimension between the overtravel stop on the jackscrew and the body of the actuator. All
measurements were consistent with the flaps being close to the fully retracted position.
70
Other deice system pneumatic lines found in the wreckage were from the center wing area, the dorsal fairing
(which extends from the lower portion of the vertical stabilizer to the top of the fuselage), the aft fuselage, and the
horizontal and vertical stabilizers.

NTSB Aircraft Accident Report
28
1.13 Medical and Pathological Information
Toxicology tests were performed by the FAA’s Civil Aerospace Medical Institute on
tissue specimens from both pilots. Specimens from the captain tested negative for ethanol. Also,
with the exception of Diltiazem,
71
his specimens tested negative for a wide range of drugs,
including major drugs of abuse (marijuana, cocaine, phencyclidine, amphetamines, and opiates).
Specimens from the first officer tested negative for ethanol and a wide range of drugs, including
major drugs of abuse.
The Erie County Medical Examiner’s Office determined that the cause of death for the
airplane occupants and the ground victim was multiple blunt force trauma.
1.14 Fire
No evidence indicated an in-flight fire. The fire damage that occurred to the airplane and
the house it impacted occurred as a result of the crash.
1.15 Survival Aspects
1.15.1 Fire Emergency Response
The Clarence Center Fire Company reported that it was the first emergency response
organization to respond to the accident scene. The fire company also reported that the following
other local emergency response organizations responded to the accident site within 15 minutes of
the accident: Niagara Airport Police, Erie County Sheriff Department, New York State Police,
Clarence Fire Company, Swormville Fire Company, and East Amherst Fire Department.
1.15.2 Natural Gas Emergency Response
About 2358 on the night of the accident, the operator of the natural gas distribution
pipeline system serving the accident area, National Fuel Gas Distribution Corporation, was
notified of blowing and burning gas at the home that was destroyed by the airplane’s impact. A
National Fuel crew truck was dispatched at 0009 on February 13, 2009, and arrived on scene
about 0033. The crew shut off the flow of gas at the homes on both sides of the accident site. The
crew was initially unable to shut off the flow of gas at the destroyed home because the gas
shutoff valve and gas meter were directly in the fire area.
About 0130, after National Fuel had completed all of the work that it could safely
accomplish, the incident commander at the accident site requested that the crew retreat from the
71
The captain’s FAA medical records indicated that he was taking this medicine to control hypertension.

NTSB Aircraft Accident Report
29
site. After 0130, National Fuel developed a plan for shutting off the flow of gas at the destroyed
home, which would have also required shutting down gas service to about 50 homes in the area
of the accident site. National Fuel discussed the plan with the Clarence Center fire chief, who,
after consultation with the incident commander, instructed National Fuel to hold off on the
shutdown because it would have required the evacuation of residents in the early morning hours
and in freezing temperatures.
About 0855, the incident commander allowed National Fuel to enter the front yard of the
destroyed home to secure the flow of gas at the home, which put out the natural gas fire. The
flow of gas into the home stopped about 1045 when the natural gas service pipeline for the home
(as well as three other homes near the accident site) was squeezed off
72
from the natural gas
distribution main pipeline. About 1320, the service pipeline was physically disconnected from
the main pipeline.
National Fuel’s investigation of the accident scene found that the fire was fed by the
natural gas service pipeline. (The natural gas distribution main pipeline was not damaged and
was subsequently returned to service.) National Fuel also found that the gas shutoff valve at the
destroyed home’s gas meter had been broken in half, causing the valve to be in the full open
position and allowing natural gas to flow and feed the fire.
In addition, National Fuel found that the service gas pipeline leading to the destroyed
home was not installed with an excess flow valve.
73
The service gas pipeline was installed in
September 1984; at the time, service pipelines were not required to be installed with an excess
flow valve.
74
Computer modeling demonstrated that, if an excess flow valve had been installed
at the destroyed home, there would have been enough gas flow for the valve to have closed and
stopped the flow of gas to the fire.
75
72
This term denotes the flattening of a plastic pipe (using a hydraulic tool) to the point at which no gas can
flow through it.
73
An excess flow valve (which is also called a gas fuse) shuts off the flow of gas if it exceeds a certain level, as
determined by the utility company that services a residence.
74
Legislation enacted in 2006 required the installation of excess flow valves after June 1, 2008, on all new and
replacement service lines to single-family residences.
75
The NTSB has issued several recommendations regarding the use of excess flow valves. For example, on
June 22, 2001, the NTSB issued Safety Recommendation P-01-2, which asked the Pipeline and Hazardous
Materials Safety Administration (which was the Research and Special Programs Administration at the time) to
require the installation of excess flow valves in all new and renewed gas service lines, regardless of customer
classification, when the operating conditions were compatible with readily available valves. Safety
Recommendation P-01-2 was classified “Open—Acceptable Response” on March 18, 2008, pending publication of
a final rule addressing integrity management for gas distribution pipelines.
NTSB Aircraft Accident Report
30
1.16 Tests and Research
1.16.1 Aircraft Performance Study
An aircraft performance study was performed to determine the time alignment among
CVR events, FDR data, and ATC radar data; calculate the airplane’s flightpath; correlate the
airplane’s position with local reference points; and examine the actions of the stall protection
system during the final portion of the flight.
Data from the FDR and a Bombardier Q400 stall protection system design document
were used to calculate the fuselage AOA during the stall sequence.
76
The calculated fuselage
AOA at the time that the autopilot disengaged was about 8°. The calculated fuselage AOA at the
time of stick shaker activation would have been about 7.6° with the ref speeds switch selected to
the increase position and about 12° with the ref speeds switch selected to the off position.
77
These AOA calculations, combined with the available CVR and FDR evidence, showed that the
ref speeds switch was in the increase position at the time of stick shaker activation.
78
Data from the FDR and the Bombardier Q400 stall protection system design document
were also used to calculate the expected low-speed cue data (with and without the ref speeds
switch set to the increase position).
79
The FDR airspeed and the calculated low-speed cue data
were then compared with the expected approach and reference speeds for the accident flight
(flaps 15, 118 knots; flaps 15 in icing conditions, 138 knots) to determine if and when the
accident airplane’s actual airspeed was below either the applicable approach speed schedule or
the low-speed cue. The comparison showed that the airspeed was below the minimum approach
speed in icing conditions for about 8 seconds before stick shaker activation and below the low-
speed cue from the initial stick shaker activation to the end of the flight.
The reference stall speeds were estimated using a flap position of 6.5°, which was the
approximate flap position at the time of the stall (based on an analysis of available FDR
parameters and an event simulation match). On the basis of an interpolation of Bombardier Q400
AFM data, the airplane would stall at 107 knots in unaccelerated (that is, a vertical acceleration
of 1 G)
80
flight for a flap position of 6.5° and an estimated landing weight of 54,700 pounds (the
approximate landing weight of the accident airplane).
81
The airplane performance study
76
Fuselage AOA is calculated from the local vane AOA using body axis pitch rate and true airspeed, among
other parameters, and is an important input to the stick shaker, stick pusher, and low-speed cue calculations.
77
The stick shaker activation angle is a function of the ref speeds switch selection, flap position, engine torque,
and Mach number.
78
The position of the ref speeds switch was not recorded by the FDR.
79
The low-speed cue is a function of engine torque, propeller speed, fuselage AOA, vertical acceleration, flap
position, calibrated airspeed, and ref speeds switch position, among other parameters.
80
G is a unit of measurement that is equivalent to the acceleration caused by the earth’s gravity
(32.174 feet/second
2
).
81
This weight did not consider the effects of ice accumulation because the flight crew had not made icing
entries into the ACARS system when transmitting the landing performance data request, as previously explained in
section 1.6.1.
NTSB Aircraft Accident Report
31
calculated that, with the extra lift required for a nose-up pitching maneuver, a Q400 airplane
with no ice accretion could achieve 1.38 Gs before encountering a wing stall at 125 knots (the
airspeed at the time that the airplane entered the stall).
82
The FDR indicated that the accident
airplane had achieved a vertical acceleration of about 1.42 Gs during the initial pitch-up
maneuver after the aft control column movement. Thus, the actual airplane performance was
slightly better than the clean wing (no ice accretion) performance assumed in the AFM.
1.16.2 Aircraft Performance Simulation Study
Bombardier Q400 aerodynamics, engine, and flight controls simulation models were used
to evaluate the accident airplane’s performance relative to the nominal airplane simulation model
(with no airframe or engine ice accumulation) and an airplane model with a degraded
performance level (which was consistent with that documented in the original certification for
the Q400 while operating within the Part 25 Appendix C icing envelope).
83
The calculated AOA,
elevator, aileron, and rudder time history values from the closed-loop event simulation
84
closely
matched the accident airplane’s motion, as documented on the FDR, during the 2-minute time
period that preceded the stall.
The Q400 simulation model contained an ice accumulation factor that ranged from 0.0,
representing a clean airplane, to 1.0, representing an airplane with ice contamination equivalent
to that demonstrated during the Q400’s certification for flight in icing conditions (per Part 25
Appendix C).
85
The NTSB found that the ice accumulation factors of 0.1 and 0.2 provided the
best match with the FDR data before the stall. The ice accumulation factor simulation results
indicated that the accident airplane experienced a small airplane performance degradation
resulting from ice accretion compared with the icing certification performance level.
The Bombardier Q400 aerodynamics, engine, and flight controls simulation models were
also used to perform a kinematics parameter extraction. This method performs a dynamic trim
calculation for each point in the data time history, with aircraft motion data (that is, linear and
angular accelerations derived from load factor and attitude data, respectively)
86
defining the trim
82
Aerodynamic stall depends on AOA and occurs at basically the same AOA regardless of load factor. A load
factor greater than 1 G, generated by either a pitch-up or turning maneuver, requires extra lift created by an
increased AOA and/or an increased airspeed. Thus, at a load factor greater than 1 G, when the stall AOA threshold
is reached, the stall occurs at a higher airspeed than with a load factor of 1 G.
83
References to Appendix C icing in this section describe performance degradations resulting from ice
accretions on Q400 unprotected surfaces and protected surfaces between boot cycles while operating in icing
conditions with the flaps at 0° and the airplane operating at holding speeds. The operational icing speed increments
were based on the Q400 icing certification flight tests.
84
A closed-loop event simulation attempts to replicate the target airplane pitch, roll, and heading angles as a
function of time by applying small increments to the nominal FDR elevator, aileron, and rudder surface position
parameters used to backdrive the airplane motion. The airplane engine settings, flap position, and gear position are
specified as a function of time.
85
In the simulation study, the Q400 aerodynamic drag and lift effects of ice accretion were incremented
linearly for ice accumulation factors between 0.0 and 1.0.
86
The load factor data include the longitudinal, lateral, and vertical acceleration parameters. The attitude data
include the airplane pitch attitude, bank angle, and heading angle parameters.
NTSB Aircraft Accident Report
32
target. The incremental aerodynamic force and moment
87
coefficients required to match the
recorded airplane motion are calculated using specific data.
88
The kinematics parameter extraction results for aerodynamic coefficients (that is,
incremental lift, drag, pitching moment, side force, rolling moment, and yawing moment)
indicated that the accident airplane did not experience any (1) linear or progressive lift
coefficient degradation over time, (2) measurable lift coefficient loss, or (3) sudden, substantial,
progressive, or sustained increase in drag coefficient (which could be clearly isolated from Q400
engine simulation and/or airplane configuration transition modeling uncertainties) for the 2-
minute time period evaluated. Only small increments in the moment coefficient values for pitch,
roll, and yaw were observed before the stall.
89
Three alternate flight control input scenarios were evaluated, with and without
performance degradation as a result of icing for three engine torque settings, to quantify the
airplane performance effects of (1) holding the control column at the expected autopilot
disengage position, (2) targeting constant pitch attitude, and (3) targeting constant altitude. The
evaluation of these alternate flight control input scenarios showed that pilot intervention was
required to avoid stalling the airplane after autopilot disconnect; that is, holding the control
column at a fixed position (the expected autopilot disengage position) and adding power would
result in the airplane continuing to increase AOA up to an aerodynamic stall. However, the Q400
simulation airplane with a conservative icing accumulation factor of 0.3 still had adequate
performance capability, with appropriate pitch axis inputs, to maintain either a constant pitch
attitude of 10° or constant altitude with engine torque values at or above the values for the
accident airplane.
In addition, the accident airplane’s fuselage AOA achieved at the peak normal load
factor
90
(13°) was compared with both the stick shaker and the stick pusher AOA schedules for
the nominal stall protection system. According to calculations provided by the supplier of the
Q400 stall protection system, the stick shaker for the accident flight condition was scheduled to
activate at a fuselage AOA of about 11.9° with the ref speeds switch selected to the off position.
The calculations also showed that the stick pusher for the accident flight condition was
scheduled to activate (after an aerodynamic stall) at a fuselage AOA of 17.5°. Because the
accident airplane achieved a peak normal load factor at a calculated fuselage AOA of about 13°,
the airplane’s AOA for maximum lift was greater than the AOA for the Q400 clean-wing stick
shaker onset (by about 1°) and was less than the AOA for the Q400 stick pusher (by about 4.5°).
87
A moment is distance multiplied by force.
88
These data are the simulation models for the airplane aerodynamics, propulsion, and flight control system;
airplane motion/state data (including altitude, airspeed, attitudes, AOA, calculated sideslip angle, and load factors);
airplane configuration (such as high-lift device and landing gear position); flight control inputs and/or control
surface positions; airplane loading (for example, weight and center-of-gravity location); and environment data
(including winds, temperature, and pressure).
89
The results after 2216:29 were subject to increased uncertainty because of uncertainties with the accident
airplane’s actual angular acceleration.
90
The peak normal load factor was achieved after autopilot disconnect but before the development of
significant bank angles.

NTSB Aircraft Accident Report
33
1.17 Organizational and Management Information
According to its website, Colgan began operations in December 1991. In July 1997, the
company began Continental Connection service through a marketing alliance and code-sharing
agreement with Continental Airlines.
91
In December 1999, Colgan started operating as a
US Airways Express carrier under a code-sharing and service agreement with US Airways. In
March 2005, Colgan resumed Continental Connection service.
92
In October 2005, the company
started providing flights for United Express under a code-sharing and service agreement with
United Airlines. In January 2007, Colgan became a wholly owned subsidiary of Pinnacle
Airlines Corporation (which was also the parent company of Pinnacle Airlines, a regional air
carrier that operated as Northwest Airlink). In February 2008, Colgan began providing
Continental Connection service out of EWR.
93
At the time of the accident, Colgan’s headquarters was located in Manassas, Virginia,
but, on December 1, 2009, the company relocated to Memphis (where Pinnacle Airlines’
headquarters is located). At the time of the accident, the company offered about 350 daily flights
to 53 cities in 15 states and Canada. Also, the company had about 1,300 employees and 34 Saab
340 and 15 Q400 airplanes (including the accident airplane) in its fleet. In February 2007,
Colgan announced the introduction of the Q400 into its fleet, and initial training of company
flight crews on the Q400 began in September 2007 at FlightSafety International’s facility in
Toronto, Canada.
94
Colgan began Q400 service in February 2008 and became fully qualified to
conduct its own training on the Q400 in July 2008.
The Colgan certificate is managed by the FAA’s Washington Flight Standards District
Office (FSDO) in Herndon, Virginia. The FAA’s operational oversight of the company is
conducted by a principal operations inspector (POI) and aircrew program managers (APM) for
the Saab 340 and the Q400. The POI and Saab 340 APM are based at the Herndon FSDO, and
the Q400 APM is based at the Teterboro, New Jersey, FSDO.
According to the Colgan vice president of administration, at the time of the accident, the
company’s minimum flight time requirement for pilot applicants was 600 hours total flight time
with 100 hours multiengine time. This vice president also stated that a pilot with 250 to 300
hours in a Part 121 operation would be a more appealing candidate than a pilot with 1,500 hours
in a general aviation airplane. The vice president further stated that, as part of a pilot applicant’s
91
According to FAA guidance, code-sharing is a marketing arrangement in which an airline (in this case,
Continental) places its designator code on flights operated by another airline (in this case, Colgan) and sells and
issues tickets for those flights. Airlines involved in code-sharing operations are required to disclose to consumers
the corporate name of the transporting carrier.
92
At an earlier point in time, Colgan’s initial marketing alliance and code-sharing agreement with Continental
had ended.
93
Colgan operates at EWR in rooms below one of the airport’s terminals. The rooms include management and
administrative offices as well as three rooms for pilots and flight attendants. One of these rooms has computers, a
bulletin board, and crew mailboxes. Another room has a kitchen area, a television, tables, and chairs. The other
room, as previously discussed in section 1.5.1, is referred to as the crew room and has couches, recliners, and a
television.
94
Colgan was authorized to outsource initial, transition, and upgrade training, and three FlightSafety
International locations, including Toronto, were permitted to conduct this training for the Q400.
NTSB Aircraft Accident Report
34
background check, the company checked the paperwork required by the Pilot Records
Improvement Act (PRIA)
95
but that many of the pilots that the company had hired did not have
previous experience with other airlines.
Colgan indicated that it revised its flight time requirements on April 30, 2009. Newly
hired pilots are now required to have 1,000 hours total flight time and 100 hours in multiengine
aircraft. Q400 captains are now required to have 3,500 hours total flight time and one of the
following: 1,000 hours as a PIC at Colgan, 1,500 hours in aircraft type, or 2,000 hours at Colgan.
Saab 340 captains are now required to have 2,500 hours total flight time and 1,000 hours at
Colgan.
1.17.1 Flight Crew Training
The Colgan Crewmember and Dispatcher Training Program Manual, page 1-7, dated
April 11, 2008, contained instructions and information for training company pilots according to
company policies and procedures, the Federal Aviation Regulations, and operations
specifications. The director of crewmember and dispatcher training
96
was responsible for
reviewing and implementing the policies and procedures in the company’s training manual. The
director was also responsible for (1) ensuring that all pilots were trained according to the airline
transport pilot practical test standards, (2) continuously reviewing the adequacy and
completeness of the program, and (3) tracking the failure rate of pilots during training and
checkrides to ensure compliance with 14 CFR 121.401(e).
97
The training manual stated the following with regard to performance standards:
Flight crewmembers will be required to receive a satisfactory grade on all flight
maneuvers, procedures and duties. A satisfactory grade is obtained ONLY when
the student demonstrates the ability to operate the aircraft/simulator in a manner
that shows he/she is obviously the master of the aircraft, and with successful
outcome of each maneuver never in doubt.
Colgan used a computer record system to maintain training records for pilots,
dispatchers, instructors, and check airmen. Paper training forms were used for grading simulator
95
PRIA records include information on accidents, incidents, violations, and drug or alcohol issues during the
previous 5 years for pilots that have worked for Part 121, 125, or 135 operators. Section 1.18.2.1 contains additional
information about PRIA. At the time of the accident, Colgan’s PRIA records were reviewed by either the
company’s human resources manager or administration vice president. PRIA records are now also reviewed by
Colgan’s flight standards or flight operations manager.
96
According to the Colgan Flight Operations Policies and Procedures Manual, the director of crewmember and
dispatcher training reports to the vice president of flight operations.
97
Title 14 CFR 121.401(e) states the following: “a person who progresses successfully through flight training,
is recommended by his instructor or a check airman, and successfully completes the appropriate flight check for a
check airman or the Administrator, need not complete the programmed hours of flight training for the particular
airplane. However, whenever the Administrator finds that 20 percent of the flight checks given at a particular
training base during the previous 6 months under this paragraph are unsuccessful, this paragraph may not be used
by the certificate holder at that base until the Administrator finds that the effectiveness of the flight training there
has improved.”
NTSB Aircraft Accident Report
35
training events and showing satisfactory completion of a training course. The course completion
information would be entered electronically into the computer training record system, and the
paper training records, including pilot grading, would then be destroyed.
98
1.17.1.1 Stall Training
Stall training for the Q400 occurs during three of eight simulator sessions during initial,
transition, upgrade, and requalification training. These three simulator sessions included three
approach-to-stall profiles—in the clean (cruise flight), takeoff, and landing configurations—that
are evaluated during a proficiency check. The company’s approach-to-stall profiles were
consistent with the FAA’s airline transport pilot practical test standards.
The simulator training events for the clean, takeoff, and landing approach-to-stall profiles
are detailed in table 2. The Colgan training manual indicated that check airmen could waive two
of the three approach-to-stall configurations when a pilot’s performance in other events indicated
a high degree of proficiency.
Table 2. Colgan Air’s Approach-to-Stall Training Events
Stall profile Entry into stall During stall Exit from stall
Clean stall
180 knots and minimum
altitude of 5,000 feet agl with
power at flight idle and gear
and flaps retracted
PF maintains altitude and
heading
PF calls “stall,” advances
power to rating detent, and
calls “check power”
PF adjusts power to
maintain 180 knots
Takeoff stall
180 knots and minimum
altitude of 5,000 feet agl with
flaps at 15°, gear down, and
power at flight idle
PF maintains altitude and
begins a 20° bank turn at
120 knots
PF calls “stall,” advances
power to rating detent, rolls
wings level, and calls “check
power”
PM calls “positive rate”
PF calls “gear up”
PM calls “V
fri
”
PF calls “flaps 0”
PF adjusts power to
maintain180 knots
98
As a result, the NTSB did not have access to the accident flight crew’s grading on simulator training events,
including the approach-to-stall profiles.
NTSB Aircraft Accident Report
36
Stall profile Entry into stall During stall Exit from stall
Landing stall
180 knots and minimum
altitude of 5,000 feet agl with
flaps at 35°, gear down, and
power at flight idle
PF maintains altitude and
heading
PF calls “stall,” advances
power to rating detent, and
calls “check power, flaps 15”
PM calls “positive rate”
PF calls “gear up.”
PM calls “V
fri
”
PF calls “flaps 0”
PF adjusts power to
maintain 180 knots
Note: PF, pilot flying; PM, pilot monitoring.
During postaccident interviews, the NTSB learned that, during the approach-to-stall
recovery exercises for initial simulator training, pilots were instructed to maintain the assigned
altitude and complete the recovery without deviating more than 100 feet above or below the
assigned altitude, which had been previously required by the practical test standards for the
checkride.
99
Some company check airmen indicated that any deviation outside of that limit
would result in a failed checkride, but other company check airmen considered this altitude
limitation to be a minimal loss of altitude (which is consistent with the current practical test
standards).
Company training personnel and Q400 check airmen stated that demonstration of the
airplane’s stick pusher system was not part of the training syllabus for simulator training at the
time of the accident. Nevertheless, one check airman indicated that he demonstrated the stick
pusher during initial simulator training. The check airman stated that most of the pilots who were
shown the pusher in the simulator would try to recover by overriding the pusher. Most of the
company pilots interviewed after the accident reported that they had not received a
demonstration of or instruction on the stick pusher.
At the public hearing for this accident, Colgan’s chief Q400 instructor testified that, after
the accident, pilots began receiving a demonstration of the stick pusher system during simulator
training. The Q400 instructor stated that pilots were set up for a stall in the landing configuration
with the autopilot on. Once the stick shaker activated, the autopilot would turn off, and the pilots
would apply back pressure to the control column so that they could feel the activation of the
stick pusher.
100
The instructor added that pilots also received a demonstration on how to
overpower the stick pusher so that they could feel the operation of the pusher.
On April 6, 2009, Colgan issued CFM Operations Bulletin 09-004, Q400 Enhanced
Flight Maneuvers Training, which described the maneuvers that would be added to initial,
upgrade, transition, and recurrent training and checkrides. The additional flight maneuvers
included new stall recovery training (recovery from stalls entered during actual flight scenarios
99
The 100-foot maximum altitude standard was consistent with other practical test standards, including those
for performance maneuvers, holding, and instrument approaches.
100
The resulting airplane motion from this control input may exceed the validated simulator envelope.

NTSB Aircraft Accident Report
37
rather than the “traditionally rigid profile based maneuver demonstration”), a stick pusher
demonstration, and unusual attitude/upset recovery training. All three stall recoveries were to be
performed by each pilot during proficiency checks, including stall conditions involving autopilot
disconnect.
NTSB investigators conducted Q400 simulator observations at FlightSafety
International’s facility in Toronto.
101
The observations were conducted using nighttime
conditions, and the temperature, winds, and altimeter settings were set to the approximate
conditions at the time of the accident. The airplane gross weight was set at 54,700 pounds (the
approximate landing weight of the accident airplane), and the airspeed bugs were set to 118
knots (V
ref
) and 114 knots (V
ga
). A clean airplane (no simulated ice) was used. FlightSafety
personnel stated their belief that scenarios in which the airplane was flown to activation of the
stick pusher and then recovered were within the capabilities of the simulator model but that
fighting against the stick pusher and not recovering would cause the simulator to be outside of its
capabilities.
102
During observations of the planned clean, takeoff, and landing approach-to-stall profiles,
the pilots in the simulator cab (the Colgan lead simulator instructor for the Q400 and the
Bombardier Q-series customer service liaison pilot) noted that the recoveries did not require
significant or dynamic control inputs to accomplish.
103
NTSB investigators noted that forward
pressure on the control column and nose-down trim were needed during the recovery and that the
numbers on the IAS display would turn red about 1 to 3 knots before the onset of the stick
shaker.
Other simulator observations were made in which the airplane, while under autopilot
control, decelerated until the stick shaker activated and the pilot flew the airplane to recovery.
Several scenarios were demonstrated with the airplane’s flaps and gear up, including one in
which the ref speeds switch was off. The stick shaker onset for this scenario occurred when the
airplane was at an airspeed of 125 knots. In a scenario in which the ref speeds switch was set to
the increase position, the stick shaker onset occurred at an airspeed of 142 knots. The stick
pusher did not activate during any of these demonstrated scenarios.
NTSB investigators noted that the recoveries did not result in unusual attitudes and that
the stick shaker ceased as airspeed increased during the recoveries. The investigators also noted
that, when the ref speeds switch was changed from the increase to the off position at stick shaker
onset, the stick shaker would immediately stop, and the low-speed cue would appear in a lower
position on the IAS display (compared with its position at stick shaker onset).
During a simulator demonstration of the ILS approach to runway 23 at BUF, the stick
shaker activated at an airspeed of 127 knots. Afterward, the pilot intentionally applied aft control
101
FlightSafety’s simulator was capable of full motion, and the motion platform was on during the
observations.
102
Bombardier subsequently stated that the post-stall onset of the stick pusher was outside the bounds of the
simulator data package the company provided to FlightSafety.
103
The altitude deviations during recovery ranged from an altitude loss of 50 feet to an altitude gain of about
120 feet.
NTSB Aircraft Accident Report
38
column movement and pulled up the airplane’s nose from 10° to 30°.
104
As the airspeed
decreased to between 105 and 110 knots, the stick pusher activated, but the nonflying pilot and
the observers were not aware of the pusher’s activation (that is, they could not tell whether the
control inputs were being made by the pilot or the pusher). The recovery was successful.
1.17.1.2 Winter Operations Training
Colgan provided its flight crews with training on winter operations during initial,
transition, and recurrent ground school. Subjects presented in this course included airplane
deicing and anti-icing procedures, checks, and responsibilities; airplane surface contamination
and its effects on performance and handling characteristics; and identification of contamination
on critical surfaces. (The accident captain and first officer last received this training during his
October 2008 transition ground training and her January 2009 recurrent ground training,
respectively.)
In addition, a training video produced in 1999 by the National Aeronautics and Space
Administration (NASA), “Icing for Regional and Corporate Pilots,” was shown during winter
operations training. The purposes of the video were to review icing fundamentals, enhance
pilots’ ability to assess hazardous icing conditions, enhance pilots’ understanding of icing effects
on the airplane’s stability and control, present strategies that pilots can use to exit a hazardous
icing encounter, and discuss supercooled large droplets.
The video also discussed the possibility of a tailplane stall, which results from an ice-
contaminated horizontal stabilizer. The video described the warning signs of a tailplane stall,
which included lightening of the controls, pitch excursions, difficulty in trimming pitch,
buffeting of the controls, and sudden nose-down pitching.
105
The video indicated that the differences between a wing stall and a tailplane stall could
be subtle but that pilots needed to properly diagnose the icing problem because the recovery
techniques for the stalls were different. According to the video, the wing stall recovery technique
requires pilots to reduce the AOA by lowering the nose, adding power, and maintaining the flap
setting, whereas the tailplane stall recovery technique requires pilots to pull back on the control
column; reduce flap setting; and, for some aircraft, reduce power.
106
The NTSB notes that, at the public hearing for this accident, a Bombardier engineering
manager testified that the Q400 was not susceptible to tailplane stalls. The Bombardier official
described the flight testing—the 0 G pushover maneuver—that was performed by Bombardier
and Transport Canada to make this determination. The Bombardier engineer explained that the
maneuver, which was conducted with ice accumulation on the airplane’s tail (with both natural
104
As with Colgan’s stick pusher demonstration in the simulator, the resulting airplane motion from this
control input may exceed the validated simulator envelope.
105
This video was part of NASA’s and the FAA’s response to previous NTSB recommendations, as discussed
in section 1.18.1.11.
106
Colgan’s training manual did not include any references to tailplane stalls or tailplane stall recovery
techniques.
NTSB Aircraft Accident Report
39
icing conditions and artificial ice shapes), involved pushing the control column forward to lower
the nose of the airplane and increase the airplane’s descent rate. The Bombardier engineer
further stated that this maneuver tested “the most severe condition” (that is, the most negative
tailplane AOA) and that the airplane showed no evidence of tailplane stall characteristics, even
at -0.2 G.
107
1.17.1.3 Remedial Training
The Colgan director of flight standards stated that pilots that failed a checkride could
retrain on the specific failure item. If the pilot passed the subsequent checkride, then no further
followup after this retraining would occur. The director also stated that, for pilots with multiple
failed checkrides, he or the flight standards manager would coordinate with the training director
to assign additional training. The director indicated that pilots could be terminated if they did not
receive the additional training and pass the checkride.
The Colgan chief pilot stated that, if a pilot were considered marginal, then he would ask
the flight standards department to have a check airman observe the pilot to ensure that his or her
performance was satisfactory. The chief pilot indicated that, at the time of the accident, the
company did not have a formal program for those pilots that were considered to be weak. In
August 2009, Colgan began a formal pilot monitoring program. Colgan stated that the program
had specific criteria and processes for entry into and exit from the program and that the flight
operations department has been reviewing and revising the program’s operation.
The Colgan director of flight standards stated that he had not tracked the accident captain
in terms of his performance. The company chief pilot stated that he was aware that the captain
had failed his initial Saab 340 upgrade training proficiency check and had to be retrained and
perform the checkride again. The chief pilot also stated that he had informed the accident captain
that his subsequent proficiency check needed to be “right on.”
1.17.1.4 Crew Resource Management Training
Colgan presented crew resource management (CRM) training during initial new hire
indoctrination training (an 8-hour class) and recurrent training (a 2-hour class).
108
The training
was taught by either a ground school instructor or the manager of crewmember and dispatcher
training, and the average class size was 12 students.
109
One of the CRM training instructors
stated that the course addressed, among other things, the relationship between flight
crewmembers and the need to indicate when pilots are not observing sterile cockpit procedures.
107
The superintendent of flight test engineering at Transport Canada testified that 0 G in the maximum landing
configuration was the Q400’s lower end structural limit. This official also stated that Transport Canada
accomplished the pushover maneuver in a controlled maneuver down to -0.1 G.
108
Videos, team-building exercises, and some case studies used during initial CRM training were not used
during recurrent CRM training.
109
Pilots and dispatchers attend CRM training at Colgan’s headquarters. Flight attendants had occasionally
attended the CRM training until their training was moved to ALB.
NTSB Aircraft Accident Report
40
Two slide presentations were included in CRM training. One presentation had 45 slides
that addressed topics including command, leadership and leadership styles, expectations and
standardization, team management, communication, situational awareness, decision-making, and
automation awareness. The other presentation had 11 slides that focused on situational
awareness.
One slide in the situational awareness presentation detailed the following operational
clues to indicate a loss of situational awareness: failing to meet targets, using undocumented
procedures, departing from standard operating procedures, violating minimums or limitations,
not flying the airplane, and not looking outside. Another slide detailed the following human
factor clues associated with a loss of situational awareness: communications, ambiguity,
unresolved discrepancies, preoccupation or distraction, and confusion or “empty feeling.” The
final slide in the presentation showed an error chain and indicated that breaking the chain
involved maintaining situational awareness, checklist discipline, and standard operating
procedures.
CRM training also included accident case studies that demonstrated good human factors
and crew interaction.
110
Also, the manager of crewmember and dispatcher training stated that the
class provided pilots with enough information to develop monitoring skills. A ground school
instructor stated that CRM training discussed that the monitoring pilot needed to be attentive and
assertive in communicating any concerns.
Colgan was in the process of revising its CRM training before the accident.
111
According
to the POI, although the company’s CRM program met the FAA’s CRM guidance (see section
1.18.1.2), he and the director of flight operations, vice president of safety and regulatory
compliance, and the director of crewmember and dispatcher training wanted additional emphasis
in several areas to make the program more robust. These areas included decision-making,
leading and following, positively communicating, and setting expectations. The POI indicated
that the new CRM training would be modeled after Continental Airlines’ advanced CRM
components and would use information from CRM programs offered at other airlines.
112
In
addition, the revised training was expected to be facilitated by line pilots (instead of a ground
school instructor or the manager of crewmember and dispatcher training) to encourage more
participation from students.
110
One case study involved the United Airlines flight 232 accident in Sioux City, Iowa. In its report on this
accident, the NTSB concluded that the airplane could not have been successfully landed on a runway because of the
loss of all hydraulic flight controls (resulting from a catastrophic separation of the stage 1 fan disk from the No. 2
engine) and that, with these circumstances, the flight crew’s performance was highly commendable and greatly
exceeded reasonable expectations. For more information, see National Transportation Safety Board, United Airlines
Flight 232, McDonnell Douglas DC-10-10, Sioux Gateway Airport, Sioux City, Iowa, July 19, 1989, Aircraft
Accident Report NTSB/AAR-90/06 (Washington, DC: NTSB, 1990).
111
Information from Colgan’s third quarter 2008 safety department review included “CRM Re-design” as an
issue and a challenge. (Colgan’s safety departments and safety programs are discussed in section 1.17.7.)
112
Information from the fourth quarter 2008 safety department review indicated that Pinnacle Airlines was also
assisting with the CRM program redesign.

NTSB Aircraft Accident Report
41
Colgan provided the NTSB with a 209-slide presentation, dated July 1, 2009, for the
revised CRM/threat and error management course.
113
The slides presented industry safety data
and trends and addressed CRM decision-making, situational awareness, communication, team
building, workload management, threat and error management, monitoring, safety culture and
safety programs, automation, fatigue, hazards associated with deviations from standard operating
procedures, the company’s “VVM” (verbalize, verify, and monitor) program, and
professionalism. Also, industry accidents and incidents, including those involving Colgan pilots,
were discussed. During the summer of 2009, Colgan began providing a 2-day CRM course to
pilots, dispatchers, flight attendants, and managers at its bases at EWR and George Bush
Intercontinental Airport (IAH), Houston, Texas. In addition to the revised CRM course, the
company’s revised Flight Operations Policies and Procedures Manual, dated September 20,
2009, contained a review of CRM/threat and error management, including discussions on error
management and descriptions of behavioral skills that are necessary for effective CRM.
1.17.1.5 Captain Leadership Training
Colgan’s captain upgrade training included a 1-day course on leadership to help
upgrading captains transition to their new role.
114
(The accident captain received this training in
October 2007 when he became a new Saab 340 captain.) The director of crewmember and
dispatcher training stated that the course focused on captains’ duties, their interaction with
different departments, and the use of CRM in their expanded work activities.
Captain leadership training included a nine-slide presentation that discussed a captain’s
authority, responsibilities, and duties; the dispatch release; logbook and maintenance
discrepancies; and cabin area and flight attendant duties. The leadership training also included
the 11 slides on situational awareness that were presented as part of indoctrination and recurrent
CRM training. The director of crewmember and dispatcher training stated that captains needed
extra emphasis on situational awareness because of the additional crewmembers that they are
responsible for overseeing. The syllabus showed that, of the 6 hours 45 minutes that had been
programmed for this training, at least 4 hours 45 minutes were dedicated to captain
administrative duties.
In addition to the training, the Colgan Flight Operations Policies and Procedures Manual
provided information about the captain’s leadership responsibilities during flight. Section 5 of
the manual, dated August 22, 2008, stated that the captain was “to maintain at all times a
businesslike environment in the cockpit that is conducive to the safe and proper conduct of the
113
The FAA’s guidance on threat and error management is contained in appendix 1 of Advisory Circular (AC)
120-90, “Line Operations Safety Audits.” (See section 1.18.2.2 for more information about this AC.) The guidance
clarifies the relationship between threat and error management and CRM, stating the following: “It is important to
clarify that TEM [threat and error management] is not crew resource management (CRM) and should not be
considered a replacement for it. TEM and CRM refer to overlapping but not equivalent activities. CRM refers
specifically to activities conducted by the crew to optimize performance. These activities include threat and error
countermeasures such as briefing, contingency planning, and monitor/cross-checking, but they also include higher-
order concepts such as leadership and establishing open communication in the cockpit. Similarly, TEM includes
crew countermeasures, but it also encompasses equipment, procedural, and regulatory countermeasures.”
114
Captain leadership training is not mandated by the FAA.

NTSB Aircraft Accident Report
42
flight.” Section 2 of the manual stated that the captain was responsible for actively promoting
and utilizing CRM while on duty.
After a new captain completed IOE, Colgan provided no further scheduled oversight of
the captain until the annual line check. After the accident, Colgan changed its policy so that all
new captains would have a line check after 6 months.
1.17.2 Flight Manuals
1.17.2.1 Reference and Approach Speeds
The Bombardier Q400 AFM, section 5, dated August 4, 1999, provided reference and
approach speed information for various configurations of the airplane. The information showed
the following for the accident airplane at its estimated landing weight:
• With flaps set at 0°, the 1.23 reference stall speed (V
SR
) was 145 knots and a
minimum of 170 knots (1.23 V
SR
plus 25 knots) during icing conditions.
115
• With flaps set at 5°, the approach speed was 133 knots and a minimum of 153 knots
(flaps 5 approach speed plus 20 knots) during icing conditions.
• With flaps set at 10°, the approach speed was 124 knots and a minimum of 144 knots
(flaps 10 approach speed plus 20 knots) during icing conditions.
• With flaps set at 15°, the V
ref
for the planned landing was 118 knots and a minimum
of 138 knots (flaps 15 V
ref
speed plus 20 knots) during icing conditions.
On March 18, 2009, Colgan issued CFM Operations Bulletin 09-003, REF SPEEDS
Switch and Speed Guidance. The bulletin set the following specific target airspeeds during the
approach phase of flight: before landing gear extension, a minimum of 180 knots; before the
final approach fix, a minimum of 160 knots; and on final approach, V
ref
plus 10 knots minus
0 knots (that is, airspeeds could deviate up to 10 knots above the V
ref
speed, but no airspeeds
below V
ref
were allowed).
1.17.2.2 Operations in Icing Conditions
The Q400 AFM, section 4.7.2, Ice Protection Procedures, dated July 13, 2005, included
the following information about operations in icing conditions:
116
• For takeoff into icing conditions, the engine intake door, windshield heat, and
propeller deice are to be turned on before takeoff, and the ref speeds switch is to be
115
The Q400 AFM contained three reference stall speeds, 1.4, 1.3, and 1.23 V
SR
, and Colgan used 1.23 V
SR
.
116
The Q400 Quick Reference Handbook, dated May 15, 2005, also contained procedures for flight into icing
conditions. Quick reference handbooks are intended for flight crew use in the cockpit.
NTSB Aircraft Accident Report
43
moved to the increase position at 400 feet agl. When airframe ice is detected, the
deice boots are to be operated in the fast mode.
• For flight before encountering icing conditions, when ice is first detected, or when a
flashing “ice detected” message appears on the engine display, the ref speeds switch
is to be moved to the increase position at the same time as the engine intake door
switches, the propeller selector, and the windshield heat are selected on. Also, the
pilot’s side window heat switches are to be turned on if ice is forming on the pilot’s
side window.
• For climb, cruise, and descent in icing conditions, the minimum airspeed is to be
maintained, the deice boots are to be operated, and wing and tail boot advisory lights
are to be monitored for normal operation.
• For holding, approach, and landing in icing conditions, the minimum airspeeds for
icing are to be maintained, the deice boots are to be operated in fast mode, and a
performance weight penalty is to be applied.
The AFM also stated that, when the airplane was no longer in icing conditions, the deice
boots should continue to be used in the fast mode until the airplane is aerodynamically clean. At
that point, the deice boots and the ref speeds switch are to be turned off, and normal airspeeds
are to resume.
In addition, several airplane systems on the Q400, including the ice protection system,
required daily checks. The Colgan CFM, section 5, “Expanded Checklist,” dated May 20, 2008,
explained that the following items were to be checked on the ice protection system: airframe
deice pressure indicator, airframe mode select switch, airframe manual select switch, propeller
selector, ref speeds switch, engine intake doors, windshield heat, and stall protection system. (A
Q400 check airman explained that this 24-hour check was normally accomplished during flight
instead of preflight.)
117
Finally, the Q400 AFM and Colgan CFM stated, in the Limitations
section, that the autopilot must be disengaged during severe icing.
On February 20, 2009, Colgan issued CFM Operations Bulletin 09-001, Speed Bugs for
Landing, Icing Definitions, and Ice Equipment Operations. The bulletin emphasized the
importance of setting the proper V
ref
bugs, especially when icing conditions might be expected;
reiterated the proper icing terminology to use with the ACARS system to ensure that the proper
ice speeds are received (from AeroData) for V
ref
and V
ga
; and introduced three levels of ice
protection.
118
The bulletin prohibited selecting the ref speeds switch to the increase position
during takeoffs, and changing the position of the ref speeds switch during landings, while the
airplane was below 1,000 feet agl. The Colgan POI stated that the company conducted
mandatory briefings about the information in the bulletin with its Q400 pilots.
117
About 2132:13, the first officer detected, while reviewing the airplane’s logbooks, that a previous flight
crew had not performed the 24-hour ice protection test. The captain responded that he had just performed the test.
118
Level one was for all flight conditions and on the ground. Level two occurred in flight with a saturated air
temperature of 5° C or colder and visible moisture or 1 mile or less visibility in clouds. Level two occurred on the
ground with a saturated air temperature of 10° C or colder and visible moisture or 1 mile or less visibility with fog.
Level two also occurred on the ground when an airplane was operating on a surface that was contaminated with
snow, ice, standing water, or slush. Level three occurred when ice accretion was visible or when the ice detected
message appeared on the engine display.

NTSB Aircraft Accident Report
44
1.17.2.3 Descent, Approach, and Before Landing Checklists
The Q400 CFM, section 5, stated that the pilot flying normally called for the descent
checklist when the airplane was descending through an altitude of 18,000 feet or at the top of the
descent if the cruise altitude was below 18,000 feet. The CFM indicated that the flying pilot was
to call for the approach checklist, with sufficient time to complete the checklist, before (1)
crossing the initial approach fix or transitioning to the initial approach phase during an
instrument approach or (2) turning onto the base leg on a visual approach. The CFM further
stated that the before landing checklist was to be performed 1 nm before the final approach fix.
The Colgan Flight Operations Policies and Procedures Manual, section 5, stated that
checklists were to be performed in the challenge-response manner with the monitoring pilot
performing and double-checking the action called for by the checklist item (as announced by the
captain).
119
The manual also stated that all pilots, while performing checklists, needed to avoid
becoming so engrossed in cockpit duties that their outside vigilance would be reduced. Further,
the manual indicated that additional information about the company’s “checklist philosophy”
was included in the Q400 CFM, but the CFM did not contain such information.
120
Colgan’s postaccident CFM Operations Bulletin 09-003 (see section 1.17.2.1) announced
that the company’s approach checklist had been changed to include a callout for the ref speeds
switch, which required a response from both flight crewmembers. The bulletin further indicated
that the decision to turn the switch to the increase or off positions during an approach should be
made before entering the initial approach phase and prohibited changing the position of the ref
speeds switch below 1,000 feet agl. (This information was also communicated in Colgan’s
postaccident CFM Operations Bulletin 09-001; see section 1.17.2.2.) In addition, CFM
Operations Bulletin 09-003 stated that, when the ref speeds switch was set to the increase
position, the only speeds that could be set were for V
ref
(ice)
and V
ga
(ice)
but that, if the ref speeds
switch was subsequently turned to the off position, the airspeed targets could be changed to V
ref
and V
ga
as long as the airplane was above 1,000 feet agl.
1.17.2.4 Approach Profile and Stabilized Approach Criteria
The Q400 CFM, section 10, dated May 20, 2008, included information for approaches
with vertical guidance. According to this information, the monitoring pilot was to advise the
flying pilot of airspeed deviations greater than ± 10 knots. The information did not include a
reminder to pilots to check the airspeed against the position of the ref speeds switch.
The Colgan Flight Operations Policies and Procedures Manual, section 5, included the
company’s stabilized approach criteria. Among these criteria was the following: below 1,000
119
After the accident, Colgan implemented an initiative to train its check airmen to evaluate the performance of
the monitoring pilot (in addition to the flying pilot) during checkrides.
120
In addition, the Flight Operations Policies and Procedures Manual indicated that a statement about
“monitoring responsibility” during the required approach briefing was explained in the expanded checklist
procedures section of the Q400 CFM, but the CFM did not contain this statement.
NTSB Aircraft Accident Report
45
feet agl in instrument meteorological conditions or 500 feet agl in VMC, the airplane is to be at
an airspeed that is not less than V
ref
and is not greater than V
ref
plus 20 knots.
1.17.3 Sterile Cockpit Procedures
Colgan’s sterile cockpit procedures are discussed as part of ground school indoctrination
training during a review of the subjects covered in the company’s Flight Operations Policies and
Procedures Manual. The manager of crewmember and dispatcher training stated that ground
school instructors referenced applicable policies and pages in the manual. (The slides presented
during indoctrination training did not include this information.) Section 3 of the manual, dated
December 20, 2007, referenced 14 CFR 121.542, “Flight Crewmember Duties,” which discusses
the sterile cockpit rule. Sections (a) through (c) of the regulation state the following:
No flight crewmember may perform any duties during a critical phase of flight
not required for the safe operation of the aircraft.
No flight crewmember may engage in, nor may any PIC permit, any activity
during a critical phase of flight which could distract any flight crewmember from
the performance of his/her duties or which could interfere in any way with the
proper conduct of those duties.
Critical phases of flight include all ground operations involving taxi (movement
of an airplane under its own power on the surface of an airport), take-off and
landing, and all other flight operations conducted below 10,000 feet MSL, except
during cruise flight.
The director of crewmember and dispatcher training stated that sterile cockpit procedures
were referenced in the flight attendant training program more than the pilot training program
because newly hired flight attendants from outside the aviation industry needed to be made
aware of the importance of not interrupting the flight crew during critical phases of flight. The
director of crewmember and dispatcher training added that pilots were instructed on the critical
phases of flight during indoctrination training.
Check airmen stated that, during checkrides, captains were expected to brief sterile
cockpit procedures before the flight, and the procedures were expected to be followed during the
flight. The company chief pilot stated that he issued a CrewTrac message in summer 2008 about
the need to adhere to rules,
121
including the sterile cockpit rule, and avoid complacency, but the
company was not able to identify any such message in response to a request from the NTSB.
122
121
CrewTrac messages are presented to pilots when they log into the company’s computer system. Pilots need
to review and acknowledge the information in the CrewTrac messages before they can check in or view their flight
schedule.
122
Colgan was asked to provide CrewTrac messages that addressed sterile cockpit adherence or standard
operating procedures and were sent to pilots based at EWR or ORF from January 2008 to the date of the accident.
No message on either topic was found.

NTSB Aircraft Accident Report
46
One first officer indicated that company pilots adhered to sterile cockpit procedures.
Another first officer indicated that captains with whom he had flown deviated rarely from sterile
cockpit procedures but that, when they did, he would speak up by redirecting them to the tasks at
hand. Check airmen and captains indicated that sterile cockpit adherence was good but that,
when the sterile cockpit rule was not being followed, they would either remind the pilot about
the rule or they would ignore the pilot’s statement to convey the message that the pilot should
not be talking. The company POI stated that FAA surveillance of Colgan before the accident (as
well as the company’s own surveillance) did not indicate a problem with crew adherence to
sterile cockpit procedures.
According to the company’s director of crewmember and dispatcher training, after the
accident, he tasked the manager of crewmember and dispatcher training with enhancing the
ground school presentations to ensure that pilots were doing their jobs and following procedures.
The manager of crewmember and dispatcher training and a ground school instructor added a
recurrent training slide that explicitly addressed adherence to sterile cockpit procedures. The
slide referenced cockpit decorum, the sterile cockpit concept, maintaining cockpit stations
(including airplane control), and preflight procedures (including the captain’s briefing and other
preflight information).
On February 26, 2009, the company chief pilot issued a CrewTrac message addressing
sterile cockpit adherence. The message defined sterile cockpit during the ascent as beginning
when the flight attendant closes the cockpit door and ending when the airplane climbs through
10,000 feet. The message defined sterile cockpit during the descent as the time from when the
airplane is descending through 10,000 feet to the completion of the parking checklist. The
message indicated, “when in sterile cockpit no extraneous conversation of any kind may take
place. Remember this also covers non essential activities such as eating.”
In October 2009, the company reported that it had added to its checklists an item for the
10,000-foot sterile cockpit period. The company further reported that it also expanded the scope
of the sterile cockpit period to include (1) 1,000 feet above or below a level-off altitude and (2)
approaching the top of descent on crossing restrictions and pilot-discretion descents.
123
1.17.4 Commuting Policy
Colgan’s Flight Crewmember Policy Handbook, dated March 2008, stated that a
commuting pilot was expected to report for duty in a timely manner. Commuting pilots were
expected to be listed in an airline reservation system aboard two separate flights that had
adequate seat availability and were scheduled to arrive at the pilot’s duty station at a reasonable
time before the pilot was scheduled to report for duty. If the pilot missed the first flight, then the
pilot was required to notify crew scheduling of the estimated time of departure for the second
flight so that plans could be made in case the second flight was missed. If the pilot missed the
123
Colgan’s September 20, 2009, revision of its Flight Operations Policies and Procedures Manual
incorporated this information.

NTSB Aircraft Accident Report
47
second flight, then the pilot was to contact crew scheduling and make every effort to report to the
location where the pilot was scheduled to begin duty.
The policy recognized that pilots might be unable to report for duty because of
unforeseen flight schedule disruptions and, as a result, provided relief from disciplinary actions
to pilots twice in any 12-month period for this reason. The policy stated that pilots who
demonstrated a pattern of missed trips would no longer be able to use the company’s commuting
policy, even if the pilot had complied with the above requirements of the policy.
The February 2006 edition of the Flight Crewmember Policy Handbook stated the
following information:
124
While commuting by Flight Crewmembers is understood and accepted by the
Company, in no way will commuting be deemed a mitigating factor in the Flight
Crewmember’s scheduling, punctuality and demeanor. All Flight Crewmembers
will be fully accountable for their timely arrival and appearance at their base. Any
and all expenses incurred because of commuting will be borne by the Flight
Crewmember. Flight Crewmembers should not attempt to commute to their base
on the same day they are scheduled to work.
This statement did not appear in the March 2008 handbook (which was the edition
current at the time of the accident).
1.17.4.1 Commuting Status of Pilots Based at Newark
During a February 2009 postaccident interview, the EWR regional chief pilot stated that
he did not know the number of commuting pilots at EWR.
125
The regional chief pilot also stated
that no restrictions were placed on pilots regarding commuting but that pilots had to meet
schedule requirements. An EWR-based first officer thought that most commuting pilots had
crash pads or shared apartments. Another EWR-based pilot stated that the reason for the large
number of commuting pilots was the high cost of living in the EWR area and the low wages that
company pilots received.
In response to an NTSB request for information, Colgan asked its 137 EWR-based pilots,
in April 2009, about their commuting status. Of these 137 pilots, 93 (68 percent) identified
themselves as commuters. Colgan also responded with address information for its EWR-based
pilots, which the NTSB cross-checked against the FAA’s airmen certification database between
April 9 and 13, 2009. Of the 137 addresses provided by Colgan, 136 were found in the FAA’s
database. Table 3 shows the geographic distribution for these 136 EWR-based pilots.
124
Colgan’s Employee Handbook, dated February 2005, contained the following similar statement about
commuting: “Colgan understands it may be necessary for employees to commute, however, in no way will
commuting be deemed a mitigating factor in an employee’s schedule, punctuality or demeanor. All employees will
be fully accountable for on time appearance at their base (for their shift). Any and all expenses incurred because of
commuting will be the responsibility of the employee.”
125
The EWR chief pilot commuted from his home in North Carolina to EWR and had a crash pad in the EWR
area.
NTSB Aircraft Accident Report
48
Table 3. Geographic Distribution of Colgan Air Pilots Based at Newark, New Jersey
Distance from EWR
(in statute miles)
Number of pilots States represented
Less than 100 45 Connecticut, New Jersey, New York, Pennsylvania
100 to 199 13 Maryland, Massachusetts, New York, Pennsylvania,
Rhode Island
200 to 399 29 Maine, Massachusetts, New Hampshire, New York,
North Carolina, Pennsylvania, Virginia
400 to 999 20 Florida, Georgia, Illinois, Iowa, Michigan, Ohio, South
Carolina, Tennessee, West Virginia
1,000 or more 29 California, Colorado, Florida, Louisiana, Minnesota,
Nevada, Texas, Utah, Washington
Note: Geographic distances from EWR were determined using the pilots’ address on record with the FAA. The number of statute
miles was based on straight-line distances between zip codes.
1.17.5 Fatigue Policy
Colgan’s fatigue policy for its pilots (and flight attendants) is addressed during basic
indoctrination ground school and is included in the Flight Operations Policies and Procedures
Manual. The fatigue policy at the time of the accident was as follows:
Colgan recognizes that there may be occasions and/or circumstances where a
Crewmember’s ability to accept or complete an assignment is altered by fatigue.
While our concerns are oriented to serve safe operations, we need to review all of
the known factors which have led to a call of Crewmember fatigue and any
resultant operations impact. This information will facilitate the development of
fatigue history and identify factors which led to fatigue. We can then evaluate
fatigue and [its] relationship to operational considerations which may improve our
planning and prevent recurrence.
When a Crewmember is unable to complete an assignment or reassignments
because of fatigue, he/she must accomplish the following:
• Immediately notify SOC [Systems Operations Control] and the Operations
Duty Officer.
• Complete the Crewmember Fatigue Form
[ ]126
…. Within 24 hours of
being released from duty because of declared fatigue, [provide] the
completed form to the Chief Pilot or Duty Officer.
The EWR regional chief pilot stated that, between May 2008 and February 2009, only
about a dozen pilots had called in fatigued. The regional chief pilot also stated that, if pilots were
fatigued, they could call in as such to crew scheduling or use sick leave.
127
In addition, the
126
Crewmembers were required to include, on the fatigue form, their duty time on the day of the fatigue call
and their flight and duty times during the 6 days preceding the fatigue call, including the number of hours of rest
before duty.
127
The Colgan Employee Handbook indicated that pilots earn 0.5 day of sick leave after 90 days of
employment with the company and then 0.5 day of sick leave each month, with a maximum carryover of 30 days.

NTSB Aircraft Accident Report
49
regional chief pilot stated his philosophy about the policy, indicating that, if a pilot’s fatigue call
was a one-time event, he would only file a report but that, if a pilot were to repetitively call in
fatigued, he would talk with that pilot to figure out what was prompting the calls. A check
airman stated that he had called in fatigued one or two times and that no followup occurred
afterward.
Colgan’s September 20, 2009, revision to its Flight Operations Policies and Procedures
Manual contained additional information about the company’s fatigue policy. According to the
manual, Colgan’s safety department was the focal point for the company’s fatigue policy to
gather information to identify fatigue and scheduling issues. As a result, crewmembers were
required to submit fatigue forms to the safety department instead of the chief pilot or duty
officer. The manual also stated, “managing fatigue is one of the most critical elements of
maintaining a safe operation. Recognizing fatigue and its effects on human performance is
important, but preventing fatigue is equally essential.”
At the time of the accident, Colgan did not provide any information to its pilots about
fatigue prevention. The manager of flight safety stated that he had been developing a pamphlet
for pilots that provided information on reasons for fatigue and industry fatigue trends. The vice
president of safety and regulatory compliance stated that the document developed by the flight
safety manager was not implemented because it focused on changing duty times and report
periods as a countermeasure to fatigue, which would not have been feasible.
The Colgan POI stated that he was aware of the company’s fatigue policy. Although the
POI did not have any specific concerns with the policy, he did state, “pilots commute … they get
up early … any regional airline tries to be as productive as possible with its folks … I’m always
concerned about that.”
128
Colgan’s revised CRM course (see section 1.17.1.4) discussed the effects of fatigue on
performance, fatigue warning signs, alertness management strategies, and accidents involving
flight crew fatigue. Also, on April 29, 2009, Colgan issued Operations Bulletin 09-001 to its
Flight Operations Policies and Procedures Manual, which addressed crewmember fatigue.
129
The
bulletin discussed the company’s fatigue policy, causes of fatigue, the recognition of fatigue and
its effects on performance, strategies to combat fatigue by effectively utilizing rest periods, and
the procedures to use if a crewmember were unable to complete an assignment because of
fatigue. The bulletin stated that any crewmember who conducted a flight when fatigued or
otherwise physically incapable of completing a flight safely would be in violation of company
policy. The bulletin emphasized, using bold face and capital letters, the following statement:
“commuting to arrive at a base with either insufficient rest to prepare for flight duties, or to
arrive with minimal time before a duty day begins is inappropriate for your responsibilities as a
professional pilot!”
The EWR regional chief pilot explained that no followup would occur after a pilot has called in sick unless the sick
leave calls became repetitive, which he defined as four calls within a 12-month period.
128
Information from Colgan’s third quarter 2008 safety department review identified “crew rest challenges” as
an issue. The information also indicated that declarations of crew fatigue were increasing.
129
The information contained in this bulletin was incorporated into the September 20, 2009, revision of the
company’s Flight Operations Policies and Procedures Manual.

NTSB Aircraft Accident Report
50
On December 30, 2009, Colgan’s director of operations issued read-and-sign memo
09-12, “Interim Fatigue Policy” to all company pilots and flight attendants. The memo stated
that, although Colgan’s nonpunitive fatigue policy had provided helpful information in
understanding scheduling issues that created fatigue among crewmembers and had resulted in
crewmembers recognizing and declaring true fatigue situations, abuse of the fatigue policy was
increasing. The memo noted the following: “in the last 2 months, the instances of fatigue calls
with no valid reason for fatigue have increased to the point where frivolous fatigue calls are now
the majority” and “frivolous use of sick policy and fatigue policy at the expense of our customers
and our operational reliability is not an acceptable practice.”
The memo contained revised fatigue policy information developed by the Colgan vice
president of safety and regulatory compliance. This interim policy, which became effective on
December 31, 2009, stated that fatigue calls would not be accepted if the crewmember had a rest
period of at least 12 hours before the start of the duty day, was returning from days off, or
wanted to use the policy for a future flight. The memo noted that the safety department would
consider mitigating circumstances preventing a rest period from being fully used when
determining whether a fatigue call was acceptable. The memo cautioned, “any further blatant
abuse of the fatigue option will be addressed as a disciplinary action, and fatigue resulting from
an improper use of rest periods or personal time off duty will be treated as missed trips.” In
addition, the memo stated that the company was working with pilot and flight attendant unions to
establish a comprehensive fatigue program, including a review board process, by February 15,
2010.
1.17.6 Crew Room Policy
The EWR regional chief pilot stated that Colgan had a policy that prohibited
crewmembers from using the crew room to sleep overnight. A May 24, 2008, read-and-sign
memo from the regional chief pilot addressed sleeping in the crew room and included the
following information:
130
If a Crew Member is based in EWR [then] you are responsible for your own
overnight accommodations. Sleeping in Operations or any crew room in EWR is
strictly prohibited and will have severe disciplinary consequences, up to and
including termination.
Company records indicated that the accident captain and the accident first officer
acknowledged receipt of this policy information.
The EWR regional chief pilot also stated that, even though the crew room was accessible
at all times, he did not know of anyone who had stayed in the crew room overnight.
131
He further
130
A first officer interviewed by the NTSB knew that Colgan had a policy against sleeping overnight in the
crew room but did not know if the policy was a written one. A check airman interviewed by the NTSB recalled the
read-and-sign memo indicating that it was not permissible to sleep overnight in the crew room.
131
One check airman stated that he had not seen any pilots sleeping overnight in the crew room. Another check
airman stated that he had stayed overnight in the crew room but only when he was traveling home the next day.
NTSB Aircraft Accident Report
51
stated that Colgan did not get involved with rest issues beyond the FAA regulations for proper
crew rest but encouraged pilots to have an appropriate place to stay overnight while in Newark.
The Colgan vice president of administration stated that commuting pilots needed to have suitable
accommodations because they would not receive adequate rest if they slept in the crew room.
She further stated that the company “can’t make someone have a crash pad, but we can certainly
make them not … sleep in the crew room.” In March 2009, the EWR regional chief pilot began
requiring that some lights remain on at all times in the crew room to ensure that pilots were not
using the room as a crash pad.
1.17.7 Safety Programs
1.17.7.1 Safety Management and Culture
The Colgan vice president of safety and regulatory compliance, who reports directly to
the president of the company, is responsible for all safety-related situations. Other Colgan
officials who are responsible for safety at the company include the director of safety and the
manager of flight safety.
132
The responsibilities of the director of safety were overseeing safety
programs, investigating and reviewing occurrences involving safety, and overseeing manual
revisions for consistency. The director of safety also attended new-hire indoctrination training to
provide an overview of the company’s safety programs. During this training, all newly hired
employees received information about submitting safety reports, contacting safety personnel,
accessing safety information on the company’s website, and finding safety information in the
company’s manuals. The responsibilities of the flight safety manager included overseeing the
aviation safety action program (ASAP), providing information for the line operations safety
audit (LOSA) program, and developing the flight operational quality assurance (FOQA)
program.
133
Colgan held quarterly safety council meetings, which were chaired by the president of the
company and included senior management personnel (at the vice president and director levels)
from all of the company’s departments. According to the company’s Safety Program Manual,
134
the purpose of the safety council meetings was to increase safety awareness, discuss unresolved
issues, facilitate group discussions, and develop positive outcomes. Colgan also held quarterly
safety review board meetings, which involved personnel at the middle management level. In
addition, safety personnel attended the company’s daily operations meetings, and safety
department reviews occurred quarterly.
132
An organizational chart in the company’s Airline Administrative Guide showed that the manager of flight
safety reported directly to this vice president, whereas the Flight Operations Policies and Procedures Manual
indicated that the manager of flight safety reported directly to the director of safety, who then reported to the vice
president of safety and regulatory compliance.
133
The ASAP, LOSA, and FOQA programs are discussed in sections 1.17.7.3 through 1.17.7.5, respectively.
134
Colgan’s Safety Program Manual outlined the company’s safety policies, procedures, and reporting
programs. The manual was issued in June 2001 and was revised in April 2002, December 2005, and June 2007.

NTSB Aircraft Accident Report
Colgan’s guiding principle regarding safety was presented in two company manuals. The
Employee Manual stated, “Safety – Our primary goal is to provide 100% safe transportation for
our customers. Safety is the first priority of Colgan. No other value or goal has priority over
safety.” The Flight Operations Policies and Procedures Manual stated, “In all aspects of
Colgan’s operation, safety shall be given primary consideration. Each and every employee is
responsible for ensuring safety in his own daily operations and shall promote safety among his
fellow employees.”
In August 2008, Colgan safety personnel (including the vice president of safety and
regulatory compliance) and the company president traveled to all company bases to present a
“safety road show” to pilots and other operational personnel. This safety briefing addressed
ASAP and LOSA and included a 31-slide presentation that discussed expectations for safety
(one of which was to operate the safest airline in the industry), industry accidents involving
organizational and management factors, and methods to prevent such accidents by ensuring that
a company safety culture existed. The presentation also discussed that a way to change safety
culture was by providing top-down guidance that is practiced and reinforced. In addition, the
presentation reviewed accidents involving error chains and included a slide that stated that the
cause of accidents was “rarely a single event, often a failure of common procedure, and
inattention to routine tasks and complacency.” The third quarter 2008 safety department review
indicated that the presentation had been provided to 525 employees at company headquarters and
bases.
After the accident, Colgan announced that it would be increasing the visibility of the
company’s safety department by having department personnel conduct monthly observations of
crew bases and observe flight crews during line operations.
The Colgan manager of flight safety stated that the safety culture at the company was
good because of programs, such as ASAP and LOSA, that allowed employees to provide
feedback and the corrective actions implemented by the company based on the feedback. This
manager added that pilots have also volunteered other information outside of the programs about
the company’s operations. The Q400 fleet manager also stated that the safety culture at the
company was good because of the safety message being conveyed throughout the company by
the company president and vice presidents. The manager of flight standards stated that the safety
road show helped to improve the company’s safety culture because it reinforced the importance
of safety and the message that everyone needed to work together. The director of flight standards
stated the following regarding the company’s safety culture: “the pilots that are out there every
day performing the job flying the airplanes around wouldn’t dream of doing anything but
keeping it a safe operation for themselves and their passengers and their flight attendants.”
The POI for Colgan stated that the safety culture at the company was “more reactive than
I’d like … not quite as proactive.” The POI indicated that the company needed more middle
management-level personnel to advance safety programs and conduct additional monitoring. He
52

NTSB Aircraft Accident Report
53
further stated that Colgan’s plans to implement the FAA’s air transportation oversight system
(ATOS) and a company safety management system (SMS) would facilitate change.
135
1.17.7.2 Safety Reporting Methods
According to the company’s Flight Operations Policies and Procedures Manual, Colgan
has a 24-hour safety hotline for employees to anonymously report any safety-related concern.
The safety hotline is a voicemail system that is directed to the vice president of safety and
regulatory compliance. The director of safety stated that no hotline calls had been received and
that the lack of calls was not an issue because employees could raise safety concerns directly
rather than anonymously.
The company also has several forms that employees can use to report a safety concern.
These forms are available in the company’s Flight Operations Policies and Procedures Manual
and on the company’s website. Once completed, these forms are routed to the vice president of
safety and regulatory compliance. One of the forms is the feedback reporting form, which can be
used to report manual errors and suggestions for improvements in addition to safety-related
concerns. Another form used to report safety concerns is the irregularity event report form. Pilots
can use this form, which is routed to the director of safety, to submit reports of events or
situations affecting the safe and efficient operation of the airplane while on the ground or during
flight. The director of safety stated that the irregularity event report form would be used for
reporting an incident or occurrence, whereas an ASAP form (discussed in section 1.17.7.3)
would be used when a pilot believed that a company policy or a Federal Aviation Regulation had
been breached.
The Colgan POI stated that, even though the company’s feedback reporting forms were
discussed in initial and recurrent ground school, pilots might not be providing enough feedback
to the company. The company’s APM for the Q400 fleet also stated his concern that pilots might
not be providing enough information to Colgan, even with the company reporting forms
available in their manuals. He indicated that he had previously told company personnel that
either pilots did not know the reporting methods that were available to them or managers were
not emphasizing the use of these reporting methods. The APM noted that the EWR regional
chief pilot had since placed company reporting forms on the flight crew website and was
encouraging their use to effect change.
Colgan’s Safety Program Manual stated that disciplinary actions would not be taken
against anyone who immediately discloses an occurrence involving safety.
135
ATOS employs a systems safety approach to air carrier oversight. SMS incorporates proactive safety
methods for air carriers to identify hazards, mitigate risk, and monitor the extent that air carriers are meeting their
objectives. ATOS and SMS are complementary and are designed to work in an integrated manner.
NTSB Aircraft Accident Report
54
1.17.7.3 Aviation Safety Action Program
Colgan’s ASAP, which began in 2005, involves company pilots, flight attendants,
dispatchers, mechanics, and ground personnel. The manager of flight safety, as the ASAP
coordinator, participates in event review committee meetings,
136
which also include the manager
of flight standards, an FAA representative, and a company pilot representative. The ASAP
coordinator manages the submission of ASAP reports, ensures that the findings from the event
review committee meetings are disseminated to the appropriate personnel for corrective action,
analyzes ASAP data each quarter to identify trends, and prepares quarterly and annual reports
that are provided to managers in the flight standards and flight operations departments and are
posted on the company’s website.
ASAP reporting forms are available on the company’s website. The ASAP form includes
a box that can be checked if the report should also be sent to NASA’s Aviation Safety Reporting
System (ASRS),
137
which is a national repository for voluntary reports regarding aviation safety-
related issues and events.
138
The Colgan manager of flight safety stated that about 25 ASAP reports were submitted
each month. This manager also recalled that the only deviations of standard operating procedures
identified in ASAP data involved overspeeds while descending. He could not recall any reports,
during the 12 months before the accident, describing problems with sterile cockpit adherence.
The company chief pilot reported that most of the ASAP data he reviewed involved altitude,
route, or clearance deviations. Company personnel stated that no ASAP reports had been
submitted before the accident regarding stall warning activations,
139
severe icing, or temporary
loss of control of an airplane. Also, the fourth quarter 2008 safety department review indicated
that ASAP trends and focus areas were runway incursions and altitude and clearance deviations.
After the accident, Colgan announced that an ASAP “reemphasis campaign” for all crew
bases would occur during summer and fall 2009. In October 2009, Colgan stated that ASAP was
being regularly emphasized to promote the program’s use; pilot participation in the program has
been “robust”; and program participation by mechanics, dispatchers, and flight attendants was
increasing. ASAP was also included as a discussion topic in the company’s revised CRM/threat
and error management training.
136
The director of safety and the vice president of safety and regulatory compliance assumed the role of ASAP
coordinator in March 2009 when the manager of flight safety left the company. A new flight safety manager was
hired in May 2009. Colgan indicated that he has emphasized the use of ASAP through base meetings and general
communications to employees.
137
Colgan uses an FAA contractor to manage the ASAP forms and the ASAP database. Colgan had asked the
contractor to change the default setting on the ASAP form so that it would not automatically be sent to the ASRS.
The company made this request after receiving feedback from pilots that the ASAP form was already similar to
other company reporting forms and that minor events, such as gate returns, were being included in the ASRS
database.
138
Because ASRS reports are submitted voluntarily, the existence of reports concerning a specific topic in the
ASRS database cannot be used to infer the prevalence of that problem within the National Airspace System.
139
A stall warning activation was reported to the ASAP database in March 2009. This event is discussed in
section 1.18.3.

NTSB Aircraft Accident Report
55
1.17.7.4 Line Operations Safety Audit
Colgan began conducting LOSA observations in 2008. The company’s manager of flight
safety stated that the purpose of these nonpunitive observations of flight deck procedures was to
identify and rectify those performance trends that deviate from standard operating procedures.
The manager of flight safety stated that “really nothing” had come up during the LOSA
observations; in particular, no problems with sterile cockpit adherence were found.
According to Colgan, company check airmen were initially used as LOSA observers
because they were already trained to be observers of operational standards. The manager of
flight safety stated that the use of check airmen for LOSA observations might raise concerns
among pilots about whether the observations were actually nonpunitive, so the company was
taking action to recruit line pilots to be LOSA observers. As of March 2009, two pilots had been
trained as LOSA observers, one who conducted observations aboard Q400 airplanes and one
who conducted observations aboard Saab 340 airplanes. The flight safety manager explained that
5 to 10 observers were needed to fully implement the LOSA program for the Q400 fleet.
After the accident, Colgan had announced that it would train LOSA observers by July
2009 and that its goal was to conduct 50 LOSA observations by September 2009. The company
did not accomplish this goal but now plans to complete a minimum of 100 LOSA observations
by the end of the first quarter of 2010.
1.17.7.5 Flight Operational Quality Assurance
FOQA programs collect, deidentify, and analyze flight data to identify and correct
possible operational risks at an air carrier. Colgan had initiated actions to establish a FOQA
program, but the program was not fully implemented at the time of the accident. After the
accident, the company announced plans to equip the Q400 fleet with quick access recorders
(QARs) and targeted program implementation for July 1, 2009.
140
The company’s director of
safety stated that the installation of this equipment required a supplemental type certificate and
that the company would finalize the schedule to equip the Q400 fleet with the recorders once the
installation was approved.
Other actions that Colgan had taken to initiate a FOQA program included identifying a
vendor to support FOQA data analysis and establishing a FOQA steering committee. This
committee consisted of personnel from the maintenance, quality control, and safety departments
and was planned to be expanded to include the flight operations department and line pilots. Also,
in a letter dated May 4, 2009, to the Air Line Pilots Association (ALPA), the Colgan vice
president of flight operations proposed including CVR data in the company’s FOQA program.
This vice president explained that overlaying flight deck communications and other sounds
140
QARs are recording units installed on aircraft to store data recorded during flight. The recorders provide
quick and easy access to a removable medium, such as an optical disk or personal computer memory card, on which
the flight information is recorded. According to the FAA, QARs have been developed to record an expanded data
frame; some of the recorders support more than 2,000 parameters at higher sample rates than FDRs.

NTSB Aircraft Accident Report
generated within the flight deck from the CVR on the visual representation provided by FDR
data would provide additional safety information for accident prevention.
In October 2009, Colgan stated that it received 14 QARs for its Q400 fleet, installed
QARs on four Q400 airplanes, and planned to install the remaining 10 QARs on Q400 airplanes
by the end of December 2009. The four currently installed QARs were being periodically
downloaded to collect data to validate flight information from the recording medium to the
ground station. The company expected to receive the FOQA ground station for analysis in
November 2009, and user training was scheduled to occur in November and December 2009.
Further, a memorandum of understanding between Colgan and ALPA was expected to be signed
by December 2009, and analysis of QAR data was expected to begin by the end of January 2010.
Colgan reported in early January 2010 that the remaining 10 QARs have been installed on Q400
airplanes and that the memorandum of understanding between Colgan and ALPA was “almost
ready” for signature.
1.17.7.6 Additional Postaccident Actions
The safety department review held after the accident included a slide titled, “Flight Ops
Actions Since Feb 12.” The slide listed actions that the company had taken or planned, which
included the following:
• increased the surveillance by check airmen throughout the Q400 fleet as part of a
“standardization push”;
• increased the presence of flight operations management at crew bases;
• required pilots to ride with a check airman after an infraction;
• required dispatchers to check the icing box on the dispatch release if icing conditions
existed in either the departure or the arrival city;
• implemented a zero-tolerance policy that holds pilots accountable for “egregious”
mistakes; and
• increased the communications flow to crews with frequent CrewTrac messages and
read-and-sign memos for each event or challenge encountered by a crew.
Also, Colgan reported that it was in the process of reviewing the top-of-descent to
touchdown phase of flight for its Saab 340 and Q400 fleets. In addition, the company also
introduced the “VVM” (verbalize, verify, and monitor) program. The VVM program was
presented as part of the company’s revised CRM/threat and error management course and was
described in the September 20, 2009, revision to the Flight Operations Policies and Procedures
Manual. The manual instructed pilots to use the VVM program “during every phase of the flight,
beginning when you arrive in the weather room until you leave the flight deck at the end of the
flight. It will help you deal effectively with the threats and errors encountered in daily
operations – frequency congestion, fatigue, distractions, etc.”
56
NTSB Aircraft Accident Report
57
1.17.7.7 Safety Communications at the Newark Base
The EWR regional chief pilot stated that one way that safety information was provided to
pilots at the base is through the CrewTrac system. Pilots at the EWR base also receive safety
information through read-and-sign memos, bulletins, and manual revisions. In addition, a safety
bulletin board is posted at EWR, and the company’s website for its flight crews contains safety
information from the safety department and the flight standards department.
1.18 Additional Information
1.18.1 Previous Safety Recommendations
1.18.1.1 Sterile Cockpit Adherence
On February 7, 2006, the NTSB issued Safety Recommendation A-06-7 as a result of the
accident involving Corporate Airlines flight 5966 in Kirksville, Missouri.
141
Safety
Recommendation A-06-7 asked the FAA to do the following:
Direct the principal operations inspectors of all 14 Code of Federal Regulations
Part 121 and 135 operators to reemphasize the importance of strict compliance
with the sterile cockpit rule.
On May 31, 2006, the FAA stated that it would issue a Safety Alert for Operators
(SAFO)
142
to address the intent of the recommendation. According to the FAA, the SAFO would
call attention to sterile cockpit rules and remind inspectors and Part 121 and 135 operators that
strict compliance with those rules was required and that breaches had contributed to at least one
recent air carrier accident.
On November 9, 2006, the NTSB acknowledged that SAFO 06004, “Approach and
Landing Accident Reduction: Sterile Cockpit, Fatigue,” had been issued on April 28, 2006,
143
with a purpose of emphasizing sterile cockpit discipline.
144
As a result, the NTSB classified
Safety Recommendation A-06-7 “Closed—Acceptable Action.”
141
For more information, see National Transportation Safety Board, Collision with Trees and Crash Short of
Runway, Corporate Airlines Flight 5966, British Aerospace BAE-J3201, N875JX, Kirksville, Missouri, October 19,
2004, Aircraft Accident Report NTSB/AAR-06/01 (Washington, DC: NTSB, 2006).
142
FAA Order 8000.87A, dated October 24, 2006, stated that a SAFO contained important, often critical,
safety information and recommended (nonregulatory) action to be taken voluntarily by the operators identified in
the SAFO. (This order replaced FAA Order 8000.87, dated August 29, 2005, which introduced SAFOs.)
143
The NTSB notes that the issuance date of the SAFO actually preceded the date of the FAA’s letter.
144
SAFO 06004 was also issued in response to Safety Recommendation A-06-11, which is discussed in section
1.18.1.5.
NTSB Aircraft Accident Report
58
1.18.1.2 Situational Awareness
On October 16, 1996, the NTSB issued Safety Recommendation A-96-106 as a result of
the accident involving American Airlines flight 965 near Cali, Colombia.
145
Safety
Recommendation A-96-106 asked the FAA to do the following:
Revise Advisory Circular 120-51B to include specific guidance on methods to
effectively train pilots to recognize cues that indicate that they have not obtained
situational awareness, and provide effective measures to obtain that awareness.
On December 11, 1998, the FAA stated that it issued Advisory Circular (AC)
146
120-51C, “Crew Resource Management Training,” on October 30, 1998. According to the FAA,
appendix 3 of the AC specifically addressed training for pilots in recognizing cues that indicate a
lack or loss of situational awareness and training in countermeasures to restore that awareness.
The AC also referenced the FAA’s February 1998 publication, Guidelines for Situational
Awareness Training, which included expanded guidance on the subject.
On March 1, 1999, the NTSB stated that the changes to AC 120-51B, which resulted in
the issuance of AC 120-51C,
147
met the intent of the recommendation. As a result, the NTSB
classified Safety Recommendation A-96-106 “Closed—Acceptable Action.”
1.18.1.3 Pilot Professionalism
On January 23, 2007, the NTSB issued Safety Recommendation A-07-8 as a result of the
accident involving Pinnacle Airlines flight 3701 in Jefferson City, Missouri.
148
Safety
Recommendation A-07-8 asked the FAA to do the following:
Work with pilot associations to develop a specific program of education for air
carrier pilots that addresses professional standards and their role in ensuring
safety of flight. The program should include associated guidance information and
references to recent accidents involving pilots acting unprofessionally or not
following standard operating procedures.
On April 13, 2007, the FAA stated that it meets routinely with training committees from
ALPA, the Air Transport Association, the Regional Airline Association, and other groups and
145
The investigation of this accident was conducted by the Aeronáutica Civil of the Government of Colombia,
with assistance from the NTSB, in accordance with the provisions of Annex 13 to the Convention on International
Civil Aviation. In September 1996, the Aeronáutica Civil issued its report on this accident and determined that its
probable causes included the flight crew’s lack of situational awareness regarding vertical navigation, proximity to
terrain, and the relative location of critical radio aids.
146
ACs are advisory and not regulatory in nature.
147
The most recent version of the AC, 120-51E, was issued on January 22, 2004.
148
For more information, see National Transportation Safety Board, Crash of Pinnacle Airlines Flight 3701,
Bombardier CL-600-2B19, N8396A, Jefferson City, Missouri, October 14, 2004, Aircraft Accident Report
NTSB/AAR-07/01 (Washington, DC: NTSB, 2007).
NTSB Aircraft Accident Report
59
that, in future meetings, the FAA would provide a copy of an information for operators (InFO)
149
message to be issued in response to Safety Recommendation A-07-6.
150
The FAA also stated
that it would discuss Safety Recommendation A-07-8 with these groups to determine an effective
approach for addressing the underlying safety issues.
On January 22, 2008, the NTSB stated that the activities described by the FAA were
appropriate actions to take after the development of an educational program that conveys the
necessary safety information has been completed. The NTSB also stated that meetings with
ALPA, the Air Transport Association, the Regional Airline Association, and other groups would
be helpful in distributing program materials or disseminating program information. Safety
Recommendation A-07-8 was classified “Open—Acceptable Response” pending completion of
these actions.
1.18.1.4 Monitoring Pilot Responsibilities
On February 27, 2007, the NTSB issued Safety Recommendation A-07-13 as a result of
the accident involving a Cessna Citation 560 in Pueblo, Colorado.
151
Safety Recommendation A-
07-13 asked the FAA to do the following:
Require that all pilot training programs be modified to contain modules that teach
and emphasize monitoring skills and workload management and include
opportunities to practice and demonstrate proficiency in these areas.
On May 17, 2007, the FAA stated that the provisions of 14 CFR Part 61 and the practical
test standards addressed the requirement for CRM in airman certification and checking. The
FAA added that it would consider identifying, in its work program, a list of required inspections
that would reemphasize, to regional office and FSDO managers, the need to validate the training
that it already required and verify its effectiveness.
On September 10, 2008, the NTSB noted that, even though current CRM regulations
addressed the issues in Safety Recommendation A-07-13, the NTSB has investigated accidents
and incidents for which improved monitoring and workload management skills might have
interrupted the chain of events that led to the accidents and thus prevented their occurrence. The
149
On October 20, 2006, the FAA issued Order 8000.91 to establish a method of sending information to
operators in a timely manner. According to the order, an InFO message contains “valuable information for operators
that should help them meet administrative requirements or certain regulatory requirements with relatively low
urgency or impact in safety.” InFO messages are not mandatory.
150
Safety Recommendation A-07-6 was also issued as a result of findings from the Pinnacle accident. The
recommendation asked the FAA to “require regional air carriers operating under 14 Code of Federal Regulations
Part 121 to provide specific guidance on expectations for professional conduct to pilots who operate nonrevenue
flights.” On January 22, 2008, the FAA stated that the InFO would discuss the circumstances of the Pinnacle
accident (a repositioning flight) and other accidents involving nonrevenue flights and would emphasize the need for
the same high standards of professionalism that are expected for revenue flights. On May 19, 2008, the NTSB
classified Safety Recommendation A-07-6 “Open—Acceptable Alternate Response.”
151
For more information, see National Transportation Safety Board, Crash During Approach to Landing,
Circuit City Stores, Inc., Cessna Citation 560, N500AT, Pueblo, Colorado, February 16, 2005, Aircraft Accident
Report NTSB/AAR-07/02 (Washington, DC: NTSB, 2007).
NTSB Aircraft Accident Report
60
NTSB stated that the FAA’s proposal to identify a list of required inspections would be
responsive to the intent of the recommendation as long as the list provided a strong emphasis on
the monitoring and workload management components of the CRM program. Safety
Recommendation A-07-13 was classified “Open—Acceptable Response” pending the
development of such a list and its incorporation into FAA work programs for regional offices
and FSDOs.
1.18.1.5 Flight Crew Fatigue
On February 7, 2006, the NTSB issued Safety Recommendation A-06-10 as a result of
the Corporate Airlines flight 5966 accident (see section 1.18.1.1). Safety Recommendation
A-06-10, which is on the NTSB’s list of Most Wanted Transportation Safety Improvements,
asked the FAA to do the following:
152
Modify and simplify the flight crew hours-of-service regulations to take into
consideration factors such as length of duty day, starting time, workload, and
other factors shown by recent research, scientific evidence, and current industry
experience to affect crew alertness.
On September 9, 2009, the FAA stated that, during the past year, it had worked with
different groups to develop an operations specification that requires a fatigue risk management
approach to mitigating fatigue for flights that exceed 16 hours. According to the FAA, the work
highlighted the need for using such an approach in ultra-long-range flights as well as commercial
flight operations. The FAA also stated that, in June 2008, it held a 3-day international
symposium that presented current scientific knowledge of fatigue in aviation.
153
The FAA
further stated that it planned the following actions: publishing the fatigue symposium
proceedings, developing ACs to address fatigue in aviation operations and provide guidance for
including a fatigue risk management system (FRMS) within an air carrier’s SMS, collecting and
analyzing crewmember fatigue data during actual flight operations, and providing guidance for
determining adequate rest periods.
In addition, the FAA stated that, in July 2009, it established an aviation rulemaking
committee on flight and duty time limitations and rest requirements for Part 121 and 135
operations. According to the FAA, the committee developed recommendations to consolidate
and replace existing regulations for Parts 121 and 135, apply current fatigue science and
information on fatigue, address the development of FRMS, and harmonize with international
152
Safety Recommendation A-06-10 superseded Safety Recommendation A-99-45, which was issued on June
1, 1999. The recommendation asked the FAA to “establish within 2 years scientifically based hours-of-service
regulations that set limits on hours of service, provide predictable work and rest schedules, and consider circadian
rhythms and human sleep and rest requirements.” Also, Safety Recommendation A-06-10 was reiterated in the
NTSB’s report on the accident involving Pinnacle Airlines flight 4712. For more information, see Runway Overrun
During Landing, Pinnacle Airlines, Inc., Flight 4712, Bombardier/Canadair Regional Jet CL600-2B19, N8905F,
Traverse City, Michigan, April 12, 2007, Aircraft Accident Report NTSB/AAR-08/02 (Washington, DC: NTSB,
2008).
153
Staff members from the NTSB gave presentations at the symposium, and Board Member Robert L. Sumwalt
was the keynote speaker.

NTSB Aircraft Accident Report
61
fatigue mitigation initiatives. The FAA stated that it was reviewing the recommendations and
that it would publish a notice of proposed rulemaking (NPRM) in December 2009 based on the
committee’s work.
On December 29, 2009, the NTSB stated that the FAA, after years of inaction, appeared
to be on the verge of taking the recommended actions with regard to flight time limitations, duty
period limits, and rest requirements for Part 121 and 135 pilots.
154
The NTSB noted that the
FAA had proposed publishing the NPRM in early 2010 but stated that the FAA had not informed
the NTSB of the specific revisions that the NPRM would include. Thus, the NTSB was not able
to determine at that time whether the revisions would fully satisfy the intent of Safety
Recommendation A-06-10. As a result, Safety Recommendation A-06-10 remained classified
“Open—Unacceptable Response” pending the publication of an NPRM proposing to mandate
the recommended actions. (The recommendation first received this classification on
November 9, 2006.)
Also, on June 12, 2008, the NTSB issued Safety Recommendations A-08-44 and -45 as a
result of previous accidents and incidents that highlighted (1) the dangers of human fatigue
within airline operations, (2) the need to address fatigue factors related to company policies and
crewmember responsibilities, and (3) the continued need for changes to flight and duty time
regulations to effectively mitigate the dangers of fatigue to aviation operations. These
recommendations asked the FAA to do the following:
155
Develop guidance, based on empirical and scientific evidence, for operators to
establish fatigue management systems, including information about the content
and implementation of these systems. (A-08-44)
Develop and use a methodology that will continually assess the effectiveness of
fatigue management systems implemented by operators, including their ability to
improve sleep and alertness, mitigate performance errors, and prevent incidents
and accidents. (A-08-45)
On August 11, 2008, the FAA stated that it had hosted a symposium on fatigue in
aviation operations to gather and make public the best available knowledge on fatigue and
154
The NTSB’s response also addressed Safety Recommendations A-94-194 and A-95-113. Safety
Recommendation A-94-194 asked the FAA to “revise the Federal Aviation Regulations contained in 14 CFR Part
135 to require that pilot flight time accumulated in all company flying conducted after revenue operations—such as
training and check flights, ferry flights and repositioning flights—be included in the crewmember’s total flight time
accrued during revenue operations.” Safety Recommendation A-95-113 asked the FAA to “finalize the review of
current flight and duty time regulations and revise the regulations, as necessary, within 1 year to ensure that flight
and duty time limitations take into consideration research findings in fatigue and sleep issues. The new regulations
should prohibit air carriers from assigning flight crews to flights conducted under 14 CFR Part 91 unless the flight
crews meet the flight and duty time limitations of 14 CFR Part 121 or other appropriate regulations.” Both of these
recommendations, which were also on the NTSB’s Most Wanted List, had been classified “Open—Unacceptable
Response.”
155
Safety Recommendation A-08-44 superseded Safety Recommendation A-06-11, which was issued as a
result of the Corporate Airlines flight 5966 accident (see section 1.18.1.1). Safety Recommendation A-06-11 asked
the FAA to “require all 14 Code of Federal Regulations Part 121 and 135 operators to incorporate fatigue-related
information similar to that being developed by the Department of Transportation Operator Fatigue Management
Program into their initial and recurrent pilot training programs; such training should address the detrimental effects
of fatigue and include strategies for avoiding fatigue and countering its effects.”

NTSB Aircraft Accident Report
62
fatigue mitigations. The FAA also stated that it was developing operations specification
guidance for fatigue management for ultra-long-range flights (that is, flights that are greater than
16 hours in duration) but did not identify any such initiatives for shorter duration domestic Part
121 operations.
On February 3, 2009, the NTSB encouraged the FAA to ensure that its planned activities
proceed at an appropriate pace and that guidance on fatigue management systems be developed
for all components of the aviation industry and not only for ultra-long-range operations. The
NTSB asked the FAA to provide a schedule indicating when guidance for other aviation
operations would be developed and issued. Safety Recommendations A-08-44 and -45 were
classified “Open—Acceptable Response” pending receipt of this schedule and one for the
development and implementation of methodologies to continually assess the effectiveness of
fatigue management systems.
In addition, on June 27, 2008, the NTSB issued Safety Recommendations A-08-19
and -20 as a result of the accident involving Delta Connection flight 6448 in Cleveland, Ohio.
156
These recommendations asked the FAA to do the following:
In cooperation with pilot unions, the Regional Airline Association, and the Air
Transport Association, develop a specific, standardized policy for 14 Code of
Federal Regulations Part 121, 135, and Part 91 subpart K operators that would
allow flight crewmembers to decline assignments or remove themselves from
duty if they were impaired by a lack of sleep. (A-08-19)
Once the fatigue policy described in Safety Recommendation A-08-19 has been
developed, require 14 Code of Federal Regulations Part 121, 135, and Part 91
subpart K operators to adopt this policy and provide, in writing, details of the
policy to their flight crewmembers, including the administrative implications of
fatigue calls. (A-08-20)
On September 26, 2008, the FAA stated that its aviation fatigue management symposium
addressed air carrier fatigue policies, including crewmembers declining flying assignments as a
result of fatigue. The FAA stated that it was actively pursuing a multiyear action plan to address
aviation fatigue, including (1) publishing symposium proceedings; (2) developing and
distributing an AC that addresses, in general terms, policy guidance in major areas of fatigue
mitigation, including crewmember scheduling and duty policies; (3) developing an AC on FRMS
that addressed, within an SMS context, all elements of a systematic approach to mitigating
aviation fatigue; (4) publishing operations specification guidance for fatigue management in
ultra-long-range flight operations; and (5) incorporating fatigue science expertise during data
collection and analysis and policy development. The FAA also stated that its plan would include
the consideration of operator policies related to crewmembers declining flight and/or duty
assignments because of fatigue and would lead to appropriate formal policy guidance.
156
For more information, see Runway Overrun During Landing, Shuttle America, Inc., Doing Business as
Delta Connection Flight 6448, Embraer ERJ-170, N862RW, Cleveland, Ohio, February 18, 2007, Aircraft Accident
Report NTSB/AAR-08/01 (Washington, DC: NTSB, 2008).

NTSB Aircraft Accident Report
63
On June 22, 2009, the NTSB stated that the FAA’s multiyear action plan to address
aviation fatigue was responsive to both recommendations. The NTSB added that a satisfactory
response to Safety Recommendation A-08-20 needed to include a requirement for operators to
implement an appropriate policy for declining assignments based on fatigue and that the
development of guidance by itself would not be sufficient. Safety Recommendations A-08-19
and -20 were classified “Open—Acceptable Response” pending the FAA’s completion of the
recommended actions.
1.18.1.6 Stall Training
On October 24, 1994, the NTSB issued Safety Recommendation A-94-173 as a result of
the accident involving United Express flight 6291 in Columbus, Ohio.
157
Safety
Recommendation A-94-173 asked the FAA to do the following:
Ensure that the training programs for 14 Code of Federal Regulations Part 135
pilots place an increased emphasis on stall warning recognition and recovery
techniques, to include stick shaker and stick pusher, during training.
On August 7, 1995, the FAA stated that it had issued Flight Standards Information
Bulletin 95-10A, “Instrument Approach Procedures and Training,” on June 26, 1995. The
bulletin directed POIs to ensure that their Part 135 operators emphasized stall warning
recognition and recovery techniques, including stick shaker and stick pusher, during training.
On November 14, 1995, the NTSB stated that Flight Standards Information Bulletin 95-
10A complied with the intent of the recommendation. As a result, Safety Recommendation A-
94-173 was classified “Closed—Acceptable Action.”
Also, on July 29, 1997, the NTSB issued Safety Recommendation A-97-47 as a result of
the ABX Air accident in Narrows, Virginia.
158
Safety Recommendation A-97-47 asked the FAA
to do the following:
Evaluate the data available on the stall characteristics of airplanes used in air
carrier service and, if appropriate, require the manufacturers and operators of
flight simulators used in air carrier pilot training to improve the fidelity of these
simulators in reproducing the stall characteristics of the airplanes they represent
to the maximum extent that is practical; then add training in recovery from stalls
with pitch attitudes at or below the horizon to the special events training programs
of air carriers.
157
For more information, see section 1.18.4 and National Transportation Safety Board, Stall and Loss of
Control on Final Approach, Atlantic Coast Airlines, Inc., United Express Flight 6291, Jetstream 4101, N304UE,
Columbus, Ohio, January 7, 1994, Aircraft Accident Report NTSB/AAR-94/07 (Washington, DC: NTSB, 1994).
158
For more information, see National Transportation Safety Board, Uncontrolled Flight Into Terrain, ABX Air
(Airborne Express), Douglas DC-8-63, N827AX, Narrows, Virginia, December 22, 1996, Aircraft Accident Report
NTSB/AAR-97/05 (Washington, DC: NTSB, 1997).

NTSB Aircraft Accident Report
64
On June 9, 1999, the FAA stated that aerodynamic stalls and approaches to stalls are
flown during aircraft certification flight testing and that sufficient data are obtained to determine
the aircraft’s stall speed at an entry rate of 1 knot per second. The FAA also stated that an
aircraft in an aerodynamic stall might handle and perform differently than the programming in
the simulator might indicate for an identical circumstance. The FAA stated that the acquisition of
data in this flight condition would have questionable accuracy and would be costly and
dangerous to acquire. The FAA noted that, even if such data existed and were incorporated into
simulators, it is unknown whether the simulators would be able to respond accurately to the data,
given the limited nature of the motion systems on even the most advanced simulators. The FAA
further stated that, to address the recommendation, it would revise the practical test standards to
require pilots to adjust pitch, bank, and power to recover from an approach to stall and would
add a note indicating, in part, that airspeed and/or altitude loss is critical at low altitudes and
must be kept to an absolute minimum.
On November 19, 1999, the NTSB stated that the ability of simulators to faithfully
replicate an airplane’s actions in some stall and stall recovery regimes could be improved. The
NTSB noted that generic simulator modules that were developed for some highly variable events
have provided useful and necessary training for pilots. The NTSB pointed out, as an example,
microburst and windshear simulator training, which provides realistic and effective training to
pilots on specific models, even though an actual encounter is likely to be significantly different.
The NTSB stated that it was disappointed that the FAA did not make changes to improve the
fidelity of simulators in reproducing stall characteristics to the maximum extent feasible. The
NTSB added that airline pilots need to be afforded this type of training so that they are fully
prepared to recover stalled aircraft. As a result, Safety Recommendation A-97-47 was classified
“Closed—Unacceptable Action.”
In addition, on January 23, 2007, the NTSB issued Safety Recommendation A-07-4 as a
result of the accident involving the Pinnacle Airlines flight 3701 accident (see section 1.18.1.3).
Safety Recommendation A-07-4 asked the FAA to do the following:
Convene a multidisciplinary panel of operational, training, and human factors
specialists to study and submit a report on methods to improve flight crew
familiarity with and response to stick pusher systems and, if warranted, establish
training requirements for stick pusher-equipped airplanes based on the findings of
this panel.
On April 13, 2007, the FAA stated that it would ask the government-industry working
group that developed the Airplane Upset Recovery Training Aid
159
to reconvene to develop
material addressing high-altitude performance issues and high-altitude stall prevention and
recovery,
160
including a discussion of stick pusher systems. The FAA also stated that, once these
159
The Airplane Upset Recovery Training Aid was issued in 1998 and was revised in August 2004 and
November 2008.
160
The response to Safety Recommendation A-07-4 also addressed the high-altitude training issues discussed
in Safety Recommendations A-07-1 and -2, which were issued as part of the Pinnacle Airlines accident
investigation.

NTSB Aircraft Accident Report
65
materials were developed, it would strongly encourage air carrier managers, trainers, and pilots
to include the materials in training programs and pilot operating manuals.
On January 22, 2008, the NTSB acknowledged the FAA’s planned actions. The NTSB
classified Safety Recommendation A-07-4 “Open—Acceptable Response” pending completion
of these actions.
1.18.1.7 Remedial Training and Additional Oversight
On May 31, 2005, the NTSB issued Safety Recommendation A-05-14 as a result of the
accident involving Federal Express flight 647 in Memphis, Tennessee.
161
Safety
Recommendation A-05-14 asked the FAA to do the following:
Require all 14 Code of Federal Regulations Part 121 air carrier operators to
establish programs for flight crewmembers who have demonstrated performance
deficiencies or experienced failures in the training environment that would require
a review of their whole performance history at the company and administer
additional oversight and training to ensure that performance deficiencies are
addressed and corrected.
On April 13, 2007, the FAA stated that it had issued SAFO 06015, “Remedial Training
for Part 121 Pilots,” on October 27, 2006. The SAFO recommended implementation and
incorporation of a voluntary remedial Part 121 pilot training module to supplement an air
carrier’s approved training program. The FAA indicated that directors of safety at Part 121 air
carriers that do not have a voluntary remedial training module for pilots should recommend such
a program to top managers at their company.
On December 12, 2007, the NTSB stated that the FAA needed to survey all Part 121
operators to determine whether they had taken the action recommended in SAFO 06015. Safety
Recommendation A-05-14 was classified “Open—Acceptable Alternate Response” pending
completion of this survey and demonstration that all Part 121 carriers had programs to address
pilot performance deficiencies or failures during training.
On April 23, 2009, the FAA issued Notice 8900.71, which discussed verification of
remedial training for Part 121 carriers. The purpose of the notice was to provide guidance to
POIs about a required inspection to determine whether their Part 121 carriers were voluntarily
complying with SAFO 06015. The notice also instructed the POIs to make a Program Tracking
and Reporting Subsystem entry within 90 days of the date of the notice for those air carriers that
had in place, or had incorporated, the SAFO’s recommended actions in the carrier’s approved
training program.
161
For more information, see National Transportation Safety Board, Hard Landing, Gear Collapse, Federal
Express Flight 647, Boeing MD-10-10F, N364FE, Memphis, Tennessee, December 18, 2003, Aircraft Accident
Report NTSB/AAR-05/01 (Washington, DC: NTSB, 2005).
NTSB Aircraft Accident Report
66
On October 30, 2009, the FAA reported that 29 of the 82 Part 121 air carriers had
remedial training programs in place. The 82 carriers included 27 regional air carriers, 6 of which
had instituted such programs. The FAA did not provide the identities of those carriers with
remedial training programs. On December 10, 2009, the FAA Administrator testified before the
Subcommittee on Aviation, U.S. Senate Committee on Commerce, Science, and Transportation,
and stated that two-thirds of the carriers without advanced qualification programs had systems in
place to identify and manage low-time pilots and pilots with persistent performance
problems. The administrator also stated that, for those carriers without such systems, additional
FAA oversight of their training and qualification programs would be conducted.
On January 27, 2010, the FAA issued a fact sheet regarding its report, Answering the Call
to Action on Airline Safety and Pilot Training.
162
The fact sheet stated that, between June and
September 2009, 85 air carriers without advanced qualification programs were inspected to
determine if they had remedial training programs that were consistent with the guidance in
SAFO 06015. The review determined that 62 air carriers had programs fully in place to meet the
guidance for remedial training programs. The fact sheet also stated that, at the time of the
review, 15 carriers had some part of a remedial training program in place and that 9 carriers had
not implemented any component of a remedial training program. The fact sheet added that, since
the time of the review, these 24 air carriers had developed remedial training programs for
pilots.
163
1.18.1.8 Pilot Records
On November 15, 1995, the NTSB issued Safety Recommendations A-95-116 through
-119 as a result of the accident involving American Eagle flight 3379 in Morrisville, North
Carolina.
164
These recommendations asked the FAA to do the following:
Require all airlines operating under 14 CFR Parts 121 and 135 and independent
facilities that train pilots for the airlines to maintain pertinent standardized
information on the quality of pilot performance in activities that assess skills,
abilities, knowledge, and judgment during training, check flights, initial operating
experience, and line checks and to use this information in quality assurance of
individual performance and of the training program. (A-95-116)
Require all airlines operating under 14 CFR Parts 121 and 135 and independent
facilities that train pilots for the airlines to provide the FAA, for incorporation
162
The FAA’s report stated that, as a result of the information that was learned at the Colgan public hearing
and subsequent congressional hearings, the Secretary of Transportation and the FAA Administrator initiated, in
June 2009, “a Call to Action on Airline Safety and Pilot Training for FAA, air carriers, and labor organizations to
jointly identify and implement safety improvements.” For more information, see
<http://www.faa.gov/library/reports/media/call_to_action_Jan2010.pdf>.
163
The NTSB notes that, although the FAA stated that 85 carriers were reviewed, the results presented were
for 86 carriers.
164
For more information, see National Transportation Safety Board, Uncontrolled Collision With Terrain,
Flagship Airlines, Inc., dba American Eagle Flight 3379, BAe Jetstream 3201, N918AE, Morrisville, North
Carolina, December 13, 1994, Aircraft Accident Report NTSB/AAR-95/07 (Washington, DC: NTSB, 1995).

NTSB Aircraft Accident Report
into a storage and retrieval system, pertinent standardized information on the
quality of pilot performance in activities that assess skills, abilities, knowledge,
and judgment during training, check flights, initial operating experience, and line
checks. (A-95-117)
Maintain a storage and retrieval system that contains pertinent standardized
information on the quality of 14 CFR Parts 121 and 135 airline pilot performance
during training in activities that assess skills, abilities, knowledge, and judgment
during training, check flights, initial operating experience, and line checks.
(A-95-118)
Require all airlines operating under 14 CFR Parts 121 and 135 to obtain
information, from the FAA’s storage and retrieval system that contains pertinent
standardized pilot training and performance information, for the purpose of
evaluating applicants for pilot positions during the pilot selection and hiring
process. The system should have appropriate privacy protections, should require
the permission of the applicant before release of the information, and should
provide for sufficient access to the records by an applicant to ensure accuracy of
the records. (A-95-119)
With regard to Safety Recommendation A-95-116, on April 17, 1998, the FAA stated
that the enactment of PRIA in 1996 addressed the NTSB’s concerns that led to the
recommendation. The FAA pointed out that air carrier training requirements are predicated on
training to proficiency and that the current record-keeping requirements thus certify a pilot’s
proficiency during training. Further, the FAA stated that the inclusion of subjective evaluations
by individual instructors, check airmen, or FAA inspectors in a pilot’s permanent record might
make a training event a punitive experience rather than one in which pilots could learn from
mistakes.
On January 3, 2000, the NTSB stated that the FAA had provided a convincing argument
about the inappropriateness of subjective information in pilot records and the possibility that
pilot training could be negatively affected. As a result, Safety Recommendation A-95-116 was
classified “Closed—Reconsidered.”
With regard to Safety Recommendations A-95-117 through -119, on February 11, 2007,
the FAA stated that the Federal Aviation Reauthorization Act of 1996 required air carriers to
obtain, maintain, and share certain specified training records of a prospective employee. The
FAA also stated that this legislation eliminated the need for the FAA to maintain a storage and
retrieval system for pilot training records.
On June 2, 1997, the NTSB stated that the legislation met the intent of the
recommendations. As a result, Safety Recommendations A-95-117 through -119 were classified
“Closed—Acceptable Alternate Action.”
67

NTSB Aircraft Accident Report
68
Also, on January 27, 2005, the NTSB issued Safety Recommendations A-05-1 and -2 as a
result of the accident involving Air Sunshine flight 527 in Treasure Cay, Great Abaco Island,
Bahamas.
165
These recommendations asked the FAA to do the following:
Require all Part 121 and 135 air carriers to obtain any notices of disapproval for
flight checks for certificates and ratings for all pilot applicants and evaluate this
information before making a hiring decision. (A-05-1)
Conduct a study to determine whether the number of flight checks a pilot can fail
should be limited and whether the existing system of providing additional training
after a notice of disapproval is adequate for pilots who have failed multiple flight
checks. On the basis of the findings of the study, establish a flight check failure
limit and modify the recheck training requirements, if necessary. (A-05-2)
With regard to Safety Recommendation A-05-1, on September 9, 2005, the FAA stated
that notices of disapproval for flight checks for certificates and ratings are not explicitly required
by PRIA. The FAA also stated that requiring all Part 121 and 135 air carriers to obtain these
notices would require FAA rulemaking or a change to the PRIA statute. According to the FAA,
some air carriers had been asking pilot applicants, as part of their preemployment screening, to
sign a consent form that permitted the FAA to release records of notices of disapproval to the air
carrier, and the FAA was, in turn, furnishing those records to the air carrier requesting them. The
FAA added that, to address the recommendation, it would amend AC 120-68, “Pilot Records
Improvement Act of 1996,” to indicate that a letter of consent signed by a pilot applicant could
be used to authorize the FAA to release records of notices of disapproval for flight checks for
certificates and ratings to an air carrier making such a request.
On November 3, 2006, the NTSB stated that the FAA’s proposal to amend AC 120-68
might be an acceptable alternate action. The NTSB also stated that, because ACs are advisory
only, the FAA should survey all operators (after the AC is revised) to determine how many
require, as a condition of employment, a pilot applicant to submit a signed consent form
permitting the FAA to release records of notices of disapproval. Safety Recommendation A-05-1
was classified “Open—Acceptable Alternate Response” pending the revision of AC 120-68 and
the survey results. (The AC was revised on November 7, 2007; see section 1.18.2.1 for
information. The survey has not been completed.)
With regard to Safety Recommendation A-05-2, on September 9, 2005, the FAA stated
that it conducted a study in 2004 to determine if a correlation existed between flight test failures
and the airmen cited in enforcement actions. The FAA stated that it found the correlation to be
“very low … less than one percent.” The FAA expressed concern about establishing a flight
check failure limit. Specifically, the FAA stated that examiners might be extremely reluctant to
find an applicant unsatisfactory as the failure limit is approached, which could result in
applicants passing flight checks who would otherwise not pass the checks.
165
For more information, see National Transportation Safety Board, In-Flight Engine Failure and Subsequent
Ditching, Air Sunshine, Inc., Flight 527, Cessna 402C, N314AB, About 7.35 Nautical Miles West-Northwest of
Treasure Cay Airport, Great Abaco Island, Bahamas, July 13, 2003, Aircraft Accident Report NTSB/AAR-04/03
(Washington, DC: NTSB, 2004).

NTSB Aircraft Accident Report
On November 3, 2006, the NTSB stated that FAA and NTSB staff held teleconferences
in January and February 2006 to discuss the type of study that would support the intent of this
recommendation. The NTSB also stated that, in March 2006, the FAA examined data from
October 1995 to October 2005 for the study. The FAA found that, during this period, almost
164,000 notices of disapproval were issued and almost 4,800 pilots had three or more flight
check failures. The NTSB further stated that it understood the FAA’s concern about imposing a
flight check failure limit. Safety Recommendation A-05-2 was classified “Open—Acceptable
Response” pending a formal written report on the study, including a description of the data
analyzed and the results found.
1.18.1.9 Air Carrier Safety Programs
On January 23, 2007, the NTSB issued Safety Recommendations A-07-9 through -11 as a
result of the accident involving Pinnacle Airlines flight 3701 (see section 1.18.1.3). These
recommendations asked the FAA to do the following:
Require that all 14 Code of Federal Regulations Part 121 operators incorporate
into their oversight programs periodic Line Operations Safety Audit observations
and methods to address and correct findings resulting from these observations.
(A-07-9)
Require that all 14 Code of Federal Regulations Part 121 operators establish
Safety Management System programs. (A-07-10)
Strongly encourage and assist all regional air carriers operating under 14 Code of
Federal Regulations Part 121 to implement an approved Aviation Safety Action
Program and an approved Flight Operational Quality Assurance program.
(A-07-11)
With regard to Safety Recommendation A-07-9, on April 13, 2007, the FAA stated that it
encouraged operators to voluntarily conduct LOSA observations and issued AC 120-90, “Line
Operations Safety Audits,” to describe the steps, resources, and procedures for conducting the
audits. The FAA noted that LOSA was not the only way for an operator to accomplish oversight
of the safety of its operations and indicated, as an example, the advanced qualification program,
which allowed most major carriers to conduct random flight checks on their flight crews. The
FAA also stated that the most effective approach for addressing this recommendation was the
effective implementation of SMS, which would include safety audits as a key element. The FAA
indicated that it had initiated a rulemaking project for SMS.
On January 22, 2008, the NTSB stated that air carriers should establish and operate a
LOSA program because of its benefits and that the program could be part of an SMS. The NTSB
also stated that the intent of the recommendation would be met if the FAA’s rulemaking project
for SMS included a requirement for LOSA programs. Safety Recommendation A-07-9 was
classified “Open—Acceptable Response” pending completion of these actions. (Additional
information on LOSA programs appears in section 1.18.2.2.)
69

NTSB Aircraft Accident Report
70
With regard to Safety Recommendation A-07-10, on April 13, 2007, the FAA noted that
the recommendation was similar to a recent amendment to Annex 6 of the International Civil
Aviation Organization (ICAO) treaty that required SMS implementation by January 1, 2009. The
FAA stated that its rulemaking project for SMS would meet the ICAO deadline and that it
planned to impose SMS requirements on Part 121 and 135 air carriers and Part 145 repair
stations. The FAA further stated that pilot project trials related to SMS implementation were
scheduled to begin in 2007.
On January 22, 2008, the NTSB acknowledged the FAA’s planned actions. Safety
Recommendation A-07-10 was classified “Open—Acceptable Response” pending a requirement
for all Part 121 air carriers to establish SMS programs. The NTSB notes that pilot project trials
related to SMS implementation began in 2007 as scheduled and that the FAA has yet to finalize
requirements and rulemaking for Part 121 and 135 air carriers and Part 145 repair stations.
With regard to Safety Recommendation A-07-11, on April 13, 2007, the FAA stated that
it encouraged all Part 121 air carriers to voluntarily implement ASAP and FOQA. The FAA also
stated that there was significant participation by regional airlines in ASAP but that few regional
airlines participated in FOQA. To encourage further participation, the FAA stated that it would
(1) make available, at no cost, a comprehensive Web-based ASAP report submission and
database management system that could be housed at the air carrier or managed by an FAA
contractor and (2) participate, during fiscal years 2007 and 2008, in conferences and seminars
sponsored by the Regional Airline Association to increase awareness of ASAP and FOQA in the
regional airline community. The FAA also stated that AC 120-92, “Introduction to Safety
Management Systems for Air Operators,”
166
identified FOQA as one of the recommended tools
that could contribute to the required safety assurance function of an SMS. The FAA further
stated that it was engaged in rulemaking that would mandate SMS and that the expected SMS
requirement, as well as the high level of industry support for SMS, could offer an increased
incentive for regional airlines to participate in FOQA.
On January 22, 2008, the NTSB stated that the programs and initiatives that the FAA
described met the intention of the recommendation. As a result, Safety Recommendation
A-07-11 was classified “Closed—Acceptable Action.” (Additional information on FOQA
programs appears in section 1.18.2.3.)
1.18.1.10 Air Carrier Oversight
On December 20, 1996, the NTSB issued Safety Recommendation A-96-163 as a result
of its investigation of the December 1995 Tower Air flight 41 accident in Jamaica, New York.
167
Safety Recommendation A-96-163 asked the FAA to do the following:
166
AC 120-92 was issued on June 22, 2006, to provide guidance for SMS program development for air carriers
and others in the aviation industry. The guidance was based on the FAA’s review of existing worldwide SMS
programs, its own internal SMS programs, and other system safety approaches.
167
For more information, see National Transportation Safety Board, Runway Departure During Attempted
Takeoff, Tower Air Flight 41, Boeing 747-136, N605FF, JFK International Airport, New York, December 20, 1995,
Aircraft Accident Report NTSB/AAR-96/04 (Washington, DC: NTSB, 1996).

NTSB Aircraft Accident Report
71
Develop, by December 31, 1997, standards for enhanced surveillance of air
carriers based on rapid growth, change, complexity, and accident/incident history;
then revise national flight standards surveillance methods, work programs,
staffing standards, and inspector staffing to accomplish the enhanced surveillance
that is identified by the new standards.
On November 24, 2004, the NTSB stated that the FAA briefed NTSB staff in
March 2004 about programs related to oversight and surveillance of air carriers, including ATOS
and the Surveillance and Evaluation Program. The NTSB indicated that, during this briefing, the
FAA stated that the risk indicators used by the Surveillance and Evaluation Program for
targeting surveillance resources included rapid growth or expansion, new or major program
changes, complexity of aircraft or new aircraft types, and accident and incident history. Because
the FAA had developed these surveillance standards, the NTSB classified Safety
Recommendation A-96-163 “Closed—Acceptable Action.”
1.18.1.11 Low-Airspeed Alerting System
On December 2, 2003, the NTSB issued Safety Recommendations A-03-53 and A-03-54
as a result of the accident involving a King Air A100 in Eveleth, Minnesota.
168
These
recommendations asked the FAA to do the following:
Convene a panel of aircraft design, aviation operations, and aviation human
factors specialists, including representatives from the National Aeronautics and
Space Administration, to determine whether a requirement for the installation of
low-airspeed alert systems in airplanes engaged in commercial operations under
14 Code of Federal Regulations Parts 121 and 135 would be feasible, and submit
a report of the panel’s findings. (A-03-53)
If the panel requested in Safety Recommendation A-03-53 determines that a
requirement for the installation of low-airspeed alert systems in airplanes engaged
in commercial operations under 14 Code of Federal Regulations Parts 121 and
135 is feasible, establish requirements for low-airspeed alert systems, based on
the findings of this panel. (A-03-54)
Although these recommendations resulted from a stall accident that did not involve icing
conditions, the NTSB reiterated the recommendations on July 10, 2006, based on preliminary
findings of an incident involving a Saab 340 airplane (operated as American Eagle flight 3008)
that experienced a loss of control during icing conditions.
169
168
For more information, see National Transportation Safety Board, Loss of Control and Impact With Terrain,
Aviation Charter, Inc., Raytheon (Beechcraft) King Air A100, N41BE, Eveleth, Minnesota, October 25, 2002,
Aircraft Accident Report NTSB/AAR-03/03 (Washington, DC: NTSB, 2003).
169
The safety recommendation letter in which the recommendations were reiterated also addressed three
similar Saab 340 incidents investigated by the Australian Transport Safety Bureau. The letter stated, “if the flight
crews had been alerted to the rapid airspeed decrease in a timely fashion, they may have been able to take corrective
action and perhaps avoid the stall.”

NTSB Aircraft Accident Report
72
On October 3, 2006, the FAA stated that it formed an internal team of experts to assess
the feasibility of a new low-airspeed alerting system. The FAA indicated that it would provide a
status update in November 2006.
On April 3, 2007, the NTSB stated that it was encouraged that the FAA had formed a
team to begin addressing the recommendations and noted that the FAA’s status update was
planned to occur in July 2007. As a result, Safety Recommendations A-03-53 and -54 were
classified “Open—Acceptable Response.” (The FAA’s status update did not occur as planned.)
1.18.1.12 Airplane Icing
On November 30, 1998, the NTSB issued Safety Recommendations A-98-90 and -107 to
the FAA and NASA, respectively, as a result of the accident involving Comair flight 3272 in
Monroe, Michigan.
170
These recommendations asked the FAA and NASA to take the following
actions along with each other as well as other interested aviation organizations:
Organize and implement an industry-wide training effort to educate
manufacturers, operators, and pilots of air carrier and general aviation
turbopropeller driven airplanes regarding the hazards of thin, possibly
imperceptible, rough ice accumulations, the importance of activating the leading
edge deicing boots as soon as the airplane enters icing conditions (for those
airplanes in which ice bridging is not a concern), and the importance of
maintaining minimum airspeeds in icing conditions.
With regard to Safety Recommendation A-98-90, on August 2, 2001, the FAA stated that
it sponsored an icing conference in February 1999 and that, as a result of the conference, NASA,
in cooperation with the FAA, produced two videos, “Tailplane Icing” and “Icing for Regional
and Corporate Pilots.”
171
According to the FAA, the tailplane icing video provided information
about ice-contaminated horizontal stabilizers, described symptoms of tailplane ice
contamination, and suggested recovery procedures. The FAA also stated that the other icing
video, which was intended for pilots of turboprop aircraft, discussed ice protection systems, ice
accretion on aircraft, the effects of ice on performance degradation and handling qualities, and
recovery techniques from a roll or pitch upset. The FAA further stated that it distributed the
videos to its regional offices and FSDOs and that it would distribute additional videos, once they
became available, to aircraft manufacturers for use in air carrier and general aviation flight
training programs.
On January 3, 2002, the NTSB stated that the production and distribution of these icing
videos met the intent of the recommendation. As a result, Safety Recommendation A-98-90 was
classified “Closed—Acceptable Action.”
170
For more information, see National Transportation Safety Board, In-Flight Icing Encounter and
Uncontrolled Collision With Terrain, Comair Flight 3272, Embraer EMB-120RT, N265CA, Monroe, Michigan,
January 9, 1997, Aircraft Accident Report NTSB/AAR-98/04 (Washington, DC: NTSB, 1998).
171
After this date, NASA produced a third icing video, as detailed in the response to Safety Recommendation
A-98-107.

NTSB Aircraft Accident Report
73
With regard to Safety Recommendation A-98-107, on March 3, 2004, NASA stated that
it completed a computer-based training module for general aviation pilots titled “A Pilots Guide
to In-Flight Icing” and three training videos for pilots titled “Icing for General Aviation Pilots,”
“Icing for Regional and Corporate Pilots,” and “Tailplane Icing.” NASA also stated that the
purpose of the training module and videos, which were developed in cooperation with the FAA,
was to educate pilots on how to operate in and avoid icing conditions.
On August 19, 2004, the NTSB stated that NASA’s work to provide training about the
hazards associated with in-flight icing conditions met the intent of the recommendation. As a
result, Safety Recommendation A-98-107 was classified “Closed—Acceptable Action.”
1.18.1.13 Weather Information for Pilots
On August 15, 1996, the NTSB issued Safety Recommendation A-96-48 as a result of its
investigation of the American Eagle flight 4184 accident in Roselawn, Indiana.
172
Safety
Recommendation A-96-48 asked the FAA to do the following:
Direct principal operations inspectors (POIs) to ensure that all 14 Code of Federal
Regulations (CFR) Part 121 air carriers require their dispatchers to provide all
pertinent information, including airman’s meteorological information (AIRMETs)
and Center Weather Advisories (CWAs), to flightcrews for preflight and in-flight
planning purposes.
On April 24, 1997, the FAA stated that it issued Flight Standards Information Bulletin for
Air Transportation 97-03 on March 17, 1997, which directed POIs to ensure that air carriers
require dispatchers to provide pertinent information, including AIRMETs and CWAs, when
appropriate, for preflight and in-flight planning purposes. The FAA also stated that the
information in the bulletin would be incorporated into FAA Order 8400.10, “Air Transportation
Operations Inspector’s Handbook.”
173
On August 20, 1997, the NTSB stated that the flight
standards information bulletin addressed the intent of the Safety Recommendation A-96-48 and
classified it “Closed—Acceptable Action.”
172
For more information, see National Transportation Safety Board, In-flight Icing Encounter and Loss of
Control, Simmons Airlines, d.b.a. American Eagle Flight 4184, Avions de Transport Regional (ATR) Model 72-212,
N401AM, Roselawn, Indiana, October 31, 1994, Aircraft Accident Report NTSB/AAR-96/01 (Washington, DC:
NTSB, 1996).
173
FAA Order 8400.10 has been superseded by FAA Order 8900.1, “Flight Standards Information
Management System.”

NTSB Aircraft Accident Report
1.18.2 Federal Aviation Administration Guidance
1.18.2.1 Pilot Records Improvement Act
On November 7, 2007, the FAA issued AC 120-68D, “Pilot Records Improvement Act of
1996.” The AC noted that PRIA (49 United States Code 44703) was enacted to ensure that air
carriers adequately investigated a pilot’s background before allowing that pilot to conduct
commercial air carrier flights. The AC also noted that a hiring employer could not place a pilot
into service until the employer obtained and reviewed the last 5 years of the pilot’s background
and other safety-related records.
The AC included information for three different audiences: the pilot applicant, hiring
employers that must request PRIA records (any Part 121, 125, or 135 operator), and former
employers that must respond to PRIA record requests (any Part 121, 125, or 135 operator or any
person that employed the applicant as a civil or public aircraft pilot). Also, the AC indicated that
it contained expanded information to address operational situations that could affect a hiring
employer’s PRIA records request compared with the previous version (AC 120-68C, dated
January 28, 2004). In addition, the AC stated that a letter of consent signed by a pilot job
applicant could be used to authorize the FAA to release records of notices of disapproval for
flight checks for certificates and ratings to an air carrier making such a request.
1.18.2.2 Line Operations Safety Audits
On April 27, 2006, the FAA issued AC 120-90, “Line Operations Safety Audits.” The
AC provided the rationale and procedures for conducting a LOSA program at an air carrier. The
AC stated that a LOSA program included the confidential collection of safety-related operational
data by expert and highly trained observers riding in the jumpseat during regularly scheduled
flights. These data are used to assess the carrier’s strengths and weaknesses to proactively
improve safety margins and prevent degradation.
The AC explained that a LOSA program is distinct from, but complementary to, a FOQA
program and an ASAP. According to the AC, FOQA and ASAP rely on outcomes to generate
data (flight parameter exceedances and adverse crew-reported events, respectively), but LOSA
samples all activities in normal operations, including successful flights, near events, and
reportable events, and notes how flight crews manage the problems they encounter. The AC also
stated that LOSA is more project-based than FOQA and ASAP (which are continuous programs)
because the full LOSA process, including advance planning, observer selection and training, data
collection, analyses, and the final report, can take between 6 and 12 months. The AC further
stated that data from any of these safety programs can be cross-referenced to guide data
collection in another one of the programs.
The AC recommended that air carriers conduct a LOSA every 3 years. The AC stated
that the data collected during a LOSA could impact almost every department at an air carrier
because the data could help (1) identify threats in the carrier’s operating environment, (2)
74

NTSB Aircraft Accident Report
75
identify threats from within the carrier’s operations, (3) assess any areas of training that are not
successfully transferring to line operations, (4) check the quality and usability of procedures, (5)
identify airplane design problems, (6) understand pilot shortcuts and workarounds, (7) assess the
prevalence and management of incident and accident precursors (that is, vertical and lateral
deviations and unstable approaches), (8) provide a baseline for organizational change, and (9)
provide a rationale for resource allocation. The LOSA program also includes briefing
management and line pilots on the audit findings detailed in the final report and implementing
and monitoring a safety change process to address the findings.
1.18.2.3 Flight Operational Quality Assurance
On April 12, 2004, the FAA issued AC 120-82, “Flight Operational Quality Assurance,”
to provide guidance for developing, implementing, and operating a FOQA program. The AC
stated that FOQA was a voluntary safety program that was designed to make commercial
aviation safer by allowing air carrier operators and their pilots to share unidentified aggregate
data with the FAA so that it could monitor industry trends in aircraft operations and target
resources to address operational risk issues. The AC advised that FOQA programs could provide
objective safety information that would not otherwise be obtainable.
The AC explained that the basis of any FOQA program was the understanding among the
FAA, air carriers, and pilots that data provided to the FAA would be kept confidential so that the
identity of reporting pilots or air carriers would remain anonymous.
174
The AC also stated that
operator FOQA programs included provisions for the identification of safety issues and the
development and implementation of corrective actions.
According to the AC, in a FOQA program, data are periodically collected from an
aircraft using a QAR or an FDR. The retrieved data are then sent to the air carrier’s FOQA office
for validation and analysis. The data can be used to evaluate or effect change in the following
areas: operational safety, aircraft performance, aircraft systems performance, flight crew
performance, company procedures, training programs, training effectiveness, aircraft design,
ATC system operation, airport operational issues, and meteorological issues. The data can also
be shared with the FAA, other air carriers, and the aviation industry.
1.18.2.4 Standard Operating Procedures
On February 27, 2003, the FAA issued AC 120-71A, “Standard Operating Procedures for
Flight Deck Crewmembers.” The AC provided advice and recommendations about developing,
implementing, and updating standard operating procedures, which, according to the AC, “are
universally recognized as basic to safe aviation operations.”
174
Specifically, data submitted to the FAA as part of a FOQA program would be protected as “voluntarily
submitted safety related data” under 14 CFR Part 193.

NTSB Aircraft Accident Report
76
The AC included an appendix addressing standard operating procedures for flight crew
monitoring and cross-checking. The appendix provided examples of standard operating
procedures that emphasized that monitoring was a primary responsibility of both flight
crewmembers. The appendix also provided examples of standard operating procedures to support
improved monitoring during vertical segments of flight (that is, climb, descent, and approach).
175
In addition, the appendix addressed standard operating procedures to support improved
monitoring of airport surface operations and automation.
1.18.3 Interview with Colgan Air Flight Crew of Burlington, Vermont, Stick
Shaker Event
On March 10, 2009, a Colgan Q400 airplane, N188WQ, was en route from EWR to
Burlington International Airport (BTV), South Burlington, Vermont, during night VMC. While
descending into BTV, the stick shaker activated, a recovery followed, and the airplane landed at
BTV without further incident. After the event, the NTSB interviewed the flight crew and the
check airman who was administering the captain’s 1-year line check at the time.
176
The captain reported that, before the event, she had been manually flying the airplane,
and her attention had been mostly focused outside of the airplane. She also reported that she
asked the first officer for the no-ice and en route ice speeds and that the deice system (level two)
had been selected.
177
The captain reported that she and the first officer (the monitoring pilot) had
programmed the no-ice speeds because she observed no indications of ice on the wings during
the descent.
The captain stated that the last airspeed she noticed before the event was about 140 knots
and that the stick shaker had activated at an airspeed of about 135 knots and an altitude of about
1,800 feet. The first officer reported that, while performing the before landing checklist, he heard
a noise, looked up, and saw that the numbers on the IAS display had turned red. The first officer
further reported that he immediately called out “airspeed” and that the captain (the flying pilot)
immediately responded by increasing power. The captain reported that she had lowered the
airplane’s nose and added full engine power (but did not reach the detent) in response. The first
officer reported that he did not notice any significant change in the airplane’s pitch when the
captain applied full power, describing the airplane as being in a “gentle descent” at the time.
175
The AC referenced a study on crew monitoring by NASA’s ASRS, which found that 75 percent of the
monitoring errors included in the study occurred while the aircraft was in a vertical phase of flight.
176
At the time of the event, the captain had been with Colgan for more than 3 years and had been flying the
Q400 for 1 year, accumulating between 800 and 1,000 hours in the airplane. The first officer had been with Colgan
about 1 year and had been flying the Q400 for about 10 months, accumulating between 450 and 500 hours in the
airplane. The check airman had flown the Q400 for 1 year and had been a check airman for 3 1/2 years.
177
The check airman reported that the captain had selected the deice system to level two when the airplane was
at an altitude of about 13,000 feet, even though the airplane was not in icing conditions at the time. (During
postaccident interviews, the captain stated that the airplane had been in icing conditions at the time and that she
planned to turn off the equipment before landing, and the first officer stated that the airplane had been in icing
conditions earlier in the flight but that icing conditions were not occurring as the airplane was maneuvering toward
the airport.) The check airman stated that selecting the deice system to level two with no icing conditions was not
standard company procedure.

NTSB Aircraft Accident Report
77
The captain stated that the low-speed cue did not come into view until the event occurred.
She also stated that, at the onset of the event, she realized that the ref speeds switch was selected
to the increase position. The first officer stated that he then pointed out the status of the ref
speeds switch. The captain reported that she asked the first officer for the ice speeds, and he told
her that V
ref
was 140 knots. She then reportedly flew the airplane at that airspeed.
The captain indicated that, after recovering the airplane, she did not execute a missed
approach because she was in control of the airplane. The first officer reported that he did not call
for a go-around because the stick shaker activation was “a very quick thing” (lasting less than 5
seconds) and the airplane had already captured the glideslope and was stable.
The check airman stated that the stick shaker had momentarily engaged just before the
airplane intercepted the glidepath. The captain added power, gaining about 150 to 200 feet, and
reestablished a stabilized approach. The flight then continued uneventfully to a landing. The
check airman stated that the last speed before the event that he recalled with certainty was 165
knots. He also stated that the airspeed was about 130 knots when the stick shaker activated and
that the low-speed cue was visible at the time.
178
He further stated that the event was “minute”
and that he did not observe the airplane in an actual stall.
The check airman indicated that the recovery appeared normal and that the remainder of
the approach was flown at airspeeds between 150 and 155 knots. The check airman stated that, if
he had been flying, he would have executed a missed approach but noted that the approach was
stabilized and that the airplane was not in an unsafe condition after the recovery.
1.18.4 Previous Related Accident
On January 7, 1994, United Express flight 6291, a Jetstream 4101, N304UE, operated by
Atlantic Coast Airlines, crashed into a storage warehouse while on an ILS final approach to Port
Columbus International Airport, Columbus, Ohio. The flight crew, the flight attendant, and two
passengers were killed, two passengers received minor injuries, and one passenger was not
injured. The airplane was destroyed.
In its final report on this accident, the NTSB made the following conclusions:
• The airplane’s autopilot maintained the airplane on the glideslope and localizer, but
the flight crew was not monitoring or maintaining airspeed.
• The first officer failed to alert the captain of the deteriorating airspeed, which was
below the minimum specified for the approach, and the operator had no specified
callouts for airspeed deviations during instrument approaches.
178
The check airman stated that, after landing, he discussed the stick shaker activation with the captain and told
her that it would have to be reported. He also informed the captain that the checkride was unsatisfactory. The check
airman stated that, besides the stick shaker event, the captain’s performance had been satisfactory with no other
airspeed control issues.

NTSB Aircraft Accident Report
78
• The stall warning system operated properly, but the captain failed to apply full power
and properly configure the airplane in a timely manner.
• The operator did not give proper consideration to the possible consequences of
pairing a newly upgraded captain with a first officer who had no experience (before
being hired by the airline 3 months before the accident) with air carrier operations.
The NTSB determined that the probable causes of the accident included (1) an
aerodynamic stall that occurred when the flight crew allowed the airspeed to decay to stall speed
and (2) an improper pilot response to the stall warning, including failing to advance the power
levers to maximum and inappropriately raising the flaps.
179
Although light-to-moderate mixed
icing conditions occurred during the approach, the NTSB concluded that airframe icing was not
a cause of the accident.
1.18.5 Gulfstream Training Academy Information
The captain attended Gulfstream Training Academy from August 2004 to April 2005.
According to its director, the academy is a comprehensive program for professional pilots who
want to gain flight time without becoming a certified flight instructor. The academy is also
directly associated with GIA.
180
Pilots entering the academy’s program are required to have
completed their instrument, commercial, and multiengine ratings and possess a current FAA
medical certificate. The academy conducts complete applicant background checks. The director
stated that some applicants enter the academy with only 200 flight hours, whereas others have
accumulated between 1,000 and 1,500 flight hours. The program duration is from 6 to 8 months.
The program begins with a 5-day IFR refresher course during which the academy
assesses the pilots’ readiness. Those pilots that do not require additional training and experience
progress through systems training, cockpit procedures training, verbal exams, and six to eight
simulator sessions in a FlightSafety BE-1900D simulator in Orlando, Florida. This training
culminates in a checkride in both the simulator and the airplane. After passing the checkrides,
the pilot is qualified to be an SIC in the BE-1900D and then transitions to initial training and
IOE. After accomplishing IOE and a line check, pilots fly with GIA for 250 hours and are
assigned reserve status or scheduled line duty as probationary pilots. Once pilots complete the
250 flight hours, they are hired by the company as full-time first officers, are placed on furlough,
or are released from the company.
GIA’s initial training program was structured to teach pilots how to operate the BE-1900
in a Part 121 environment. As a result, the training focused on systems and procedures and not
basic flying skills, which should have been learned while pilots were completing their instrument
rating and commercial certificate.
179
Safety Recommendation A-94-173, which was issued as a result of this accident, is discussed in section
1.18.1.6.
180
According to Gulfstream Training Academy’s website, GIA is a regional air carrier with more than 200
scheduled daily flights within Florida and to the Bahamas.

NTSB Aircraft Accident Report
The captain completed initial training and, in December 2004, began flying the BE-1900
for GIA as a fully qualified first officer. GIA maintained comprehensive training records for the
captain. His training records showed that, even though he completed all entry, training, and
operating phases without a failure, the captain had experienced continuing difficulties with
aircraft control. For example, during simulator periods 3 and 4, the captain was graded
unsatisfactory in “approach to stall – landing configuration,” although he received a satisfactory
grade in later sessions. During simulator period 7, the captain’s altitude and airspeed control was
unacceptable, and comments included, “airspeed more than 10 knots below Vref + 10. Fly
correct airspeed!” “airspeed 10 knots below Vref crossing threshold,” “gear remains up during
entire approach,” and “repeated deviation from altitude 200-300 feet.”
During simulator period 8, the instructor noted, “basic attitude flying cause of repeated
deviations,” “constant deviations up to full scale on glide slope,” and “additional training
required.” All maneuvers were graded satisfactory the next day (by the same instructor as the
day before) during an extra ninth simulator period, and the simulator checkride was completed
that same day.
The captain completed his IOE at GIA in 34.8 hours, and training captains made several
positive remarks, such as “good progress,” “getting better,” and “good job, signed off from
IOE.” No further comments appeared in the captain’s GIA file about his performance while
flying as a first officer.
When the captain completed his 250 flight hours in April 2005, GIA was not hiring
pilots. According to GIA’s director of operations, the captain would have been eligible for hiring
based on his record. However, the director pointed out that, to be hired, pilots must have at least
three letters of recommendation from captains in their file, and no such letters were found for the
captain.
79

NTSB Aircraft Accident Report
2. Analysis
2.1 General
The pilots were properly certificated and qualified in accordance with applicable Federal
regulations. The airplane was properly certified, equipped, and maintained in accordance with
Federal regulations. The recovered components showed no evidence of any preimpact structural,
engine, or system failures, including no indications of any problems with the airplane’s ice
protection system.
The air traffic controllers who were responsible for the flight during its approach to BUF
performed their duties properly and responded immediately and appropriately to the loss of radio
and radar contact with the flight. Although PIREPs before the time of the accident could have
provided additional real-time information of the flight conditions on approach to BUF, no
evidence showed that the icing conditions that existed were abnormal for wintertime operations
in the BUF area. Also, the NTSB’s postaccident survey of pilots operating into BUF about the
time of the accident indicated that they were not surprised by the icing conditions and did not
consider the conditions to be significant.
This accident was not survivable.
This analysis discusses the following information:
• the accident sequence, including the minimal effect of icing on the airplane’s
performance, the flight crew’s failure to monitor airspeed in relation to the rising
position of the low-speed cue, and the captain’s incorrect actions in response to the
stall warning;
• strategies to prevent flight crew monitoring failures, including explicit pilot training
for monitoring and standard operating procedures that promote effective monitoring;
• pilot professionalism, including captain leadership skills and adherence to sterile
cockpit and standard operating procedures;
• fatigue, including commuting pilots’ use of company crew rooms as rest facilities and
industry efforts to mitigate fatigue;
• remedial training for poor-performing pilots, the need for detailed documentation of
pilot training and checking events and retention of such records, and the information
to be included in an air carrier’s assessment of a pilot applicant;
• flight crew procedures and training to ensure that selected airspeeds are matched to
the position of a ref speeds switch or similar device;
80

NTSB Aircraft Accident Report
81
• stall training that involves fully developed stall profiles (in addition to the approach-
to-stall profiles that are currently required) and a demonstration of the stick pusher
system;
• the FAA’s oversight of Colgan, including the surveillance provided at the time that
the company incorporated the Q400 into its fleet;
• flight operational quality assurance programs, including the use of downloaded safety
information to identify deviations from established norms and procedures;
• the use of personal portable electronic devices on the flight deck;
• the FAA’s use of SAFOs, which are advisory in nature, to transmit safety-critical
information; and
• preflight weather documents provided to flight crews and icing terminology presented
in an FAA publication used by pilots for basic flight information.
2.2 Accident Sequence
2.2.1 Overview
The FDR recorded the activation of the airframe and propeller deice equipment while the
airplane was climbing to its assigned cruise altitude of 16,000 feet. At that time, the captain
would have turned the ref speeds switch (on the ice protection panel above his seat) to the
increase position. According to the Bombardier Q400 AFM, the ref speeds switch was to be set
to the increase position before an airplane entered icing conditions (or upon initial detection of
icing) and was to be set to the off position when the airplane was aerodynamically clean (that is,
all ice was removed from the visible leading edges of the wing and wing tips).
For the accident airplane, turning the ref speeds switch from the off to the increase
position lowered the AOA reference for stick shaker activation and raised the position of the
low-speed cue on the pilots’ IAS displays by about 15 knots. As a result, the airplane would have
the same (or greater) performance margins relative to the stall speed during operations in icing
conditions as it would have with a clean configuration as long as the landing airspeeds were
appropriately increased to remain above the stall warning threshold.
181
The first officer had received the BUF ATIS by 2150:42 and had entered planned landing
information, including the intended runway and the airplane’s landing weight, into ACARS for
transmittal to AeroData (see section 1.6.1) for landing performance data. However, she did not
enter the keywords “icing” or “eice,” despite the icing conditions at the time, the deicing
equipment in use, the ref speeds switch in the increase position, and the expected landing
conditions (based on the ATIS information). ACARS returned the AeroData landing
181
The performance margins for operations in icing conditions were based on the worst-case ice accretions
examined during icing certification. Ice accretions with less severe performance penalties than the worst-case ice
accretions would result in a greater margin to stall.

NTSB Aircraft Accident Report
82
performance data to the airplane at 2153:00, showing a V
ref
of 118 knots and a V
ga
of 114 knots,
but these speeds were not appropriate for an airplane configured for flight in icing conditions. (If
the first officer had entered either “icing” or “eice,” then the V
ref
would have been 138 knots,
which would have included a 20-knot icing increment.) The first officer provided the speeds to
the captain, and he did not challenge them.
Variable periods of snow and light-to-moderate icing were present during the accident
airplane’s approach to BUF, and some ice accumulation was likely present on the airplane.
However, FDR data and airplane performance models showed that the airplane responded to
control inputs as expected, given the calculated ice accretion at the time, until the wing stalled.
The CVR recorded the activation of the stick shaker about 2216:27, and FDR data
showed that the activation occurred at an AOA of about 8°, a load factor of 1 G, and an airspeed
of 131 knots, which was consistent with the AOA, airspeed, and low-speed cue during normal
operations when the ref speeds switch was selected to the increase position. The airplane was not
close to stalling at the time. However, because the ref speeds switch was selected to the increase
(icing conditions) position, the stall warning occurred at an airspeed that was 15 knots higher
than would be expected for a Q400 in a clean (no ice accretion) configuration. Stick shakers
generally provide pilots with a 5- to 7-knot warning of an impending stall; thus, as a result of the
15-knot increase from the ref speeds switch, the accident flight crew had a 20- to 22-knot
warning of a potential stall.
182
CVR and FDR data indicated that, when the stick shaker activated, the autopilot
disconnected automatically. The captain responded by applying a 37-pound pull force to the
control column, which resulted in an airplane-nose-up elevator deflection, and adding power. In
response to the aft control column movement, the AOA increased to 13°, pitch attitude increased
to about 18°, load factor increased from 1.0 to about 1.4 Gs, and airspeed slowed to 125 knots. In
addition, the speed at which a stall would occur increased.
183
The airflow over the wing
separated as the stall AOA was exceeded, leading to an aerodynamic stall and a left-wing-down
roll that eventually reached 45°, despite opposing flight control inputs. Thus, the NTSB
concludes that the captain’s inappropriate aft control column inputs in response to the stick
shaker caused the airplane’s wing to stall.
The airplane experienced several roll oscillations during the wing aerodynamic stall.
FDR data showed that, after the roll angle had reached 45° left wing down, the airplane rolled
back to the right through wings level. After the first stick pusher activation, the captain applied a
41-pound pull force to the control column, and the roll angle reached 105° right wing down.
After the second stick pusher activation, the captain applied a 90-pound pull force, and the roll
angle reached about 35° left wing down and then 100° right wing down. After the third stick
pusher activation, the captain applied a 160-pound pull force. The final roll angle position
182
The airspeed at which an airplane would stall can be increased if the airplane experiences measurable loads
(that is, variation from a 1 G load) because of, for example, maneuvering or external forces. The increased stall
speed with loads greater than 1 G would erode the stall warning margin.
183
Numerous combinations of airspeed and load factor can result in the stall AOA being exceeded. The stall
warning margin that existed at the time of stick shaker activation was consumed by the increase in load factor
during the pull-up maneuver, leading to the stall AOA being exceeded at an airspeed that was much higher than the
1 G stall speed.

NTSB Aircraft Accident Report
83
recorded on the FDR was about 25° right wing down. At that time, the airplane was pitched
about 25° airplane nose down.
The airplane performance study and simulations showed that the airplane experienced
minimal performance degradation because of ice accretion.
184
Specifically, the AOA at the time
of the wing stall was about 1° above the expected AOA for a clean wing (no ice accretion) stall
warning. Thus, the airplane could have been operated in normal flight, at the non-icing V
ref
, and
with a substantial margin remaining above the actual point of stall. As a result, the NTSB
concludes that the minimal aircraft performance degradation resulting from ice accumulation did
not affect the flight crew’s ability to fly and control the airplane. The flight crew’s actions during
the accident sequence are further discussed in sections 2.2.2 through 2.2.4.
2.2.2 Approach to Airport
The approach phase of flight is dynamic and requires heightened vigilance because it
typically involves changes in the airplane’s altitude, heading, speed, and configuration. The
captain, as the flying pilot, had the primary responsibility to monitor the instruments, and the
first officer, as the monitoring pilot, was responsible for providing backup and corrective input to
the captain’s efforts.
About 2215:14, the controller informed the flight crew that the airplane was 3 miles from
the outer marker and cleared the flight for the ILS runway 23 approach. The glideslope intercept
point, as shown on the approach chart, was outside the outer marker. According to Colgan’s
guidance, the airspeed at the time (184 knots) was too fast for the airplane’s position relative to
the glideslope;
185
as a result, the captain needed to initiate a rapid slowdown less than 3 miles
from the outer marker. ATC requirements at busy airports, such as EWR (where both pilots were
based), often necessitate such a maneuver. However, in this case, it is likely that the captain had
to slow the airplane quickly because he was distracted by his conversation with the first officer
and had lost positional awareness.
186
A rapid slowdown is not unusual and is not unsafe if it is
flown properly.
187
The captain slowed the airplane by extending flaps to 5°, reducing power to
near idle,
188
extending the landing gear, and moving the condition levers to maximum rpm.
189
184
The aircraft performance simulation study results for constant pitch attitude and constant altitude (see
section 1.16.2) provide specific evidence showing that the airplane had more-than-adequate performance capability
to return to a safe flight condition.
185
The 184-knot airspeed was 46 knots faster than Colgan’s maximum allowable approach speed on the
glideslope, which is V
ref
plus 20 knots (in this case, 138 knots).
186
Air traffic was reported to be light at BUF at the time of the accident flight, and ATC had not issued any
speed restrictions for the flight.
187
Several of the 13 previous flights recorded by the FDR had involved rapid slowdowns. The Colgan Q400
APM stated that a good technique for slowing an airplane rapidly is to increase the propeller rpm.
188
The primary power indication, torque, was displayed at the top of the engine display, which would have
been in the direct view of the pilots. The power levers, which were being manipulated by the captain, were located
on the center console.
NTSB Aircraft Accident Report
84
Airspeed indications were displayed on the pilots’ PFDs, as shown previously in figure 1.
A vertical scale on the left side of each PFD showed the current airspeed (depicted in the center
of the scale) and a range of ± 42 knots from the actual airspeed, and an airspeed trend vector
predicted the airspeed at which the airplane would be flying in 10 seconds. The low-speed cue,
consisting of alternating red and black bars, appeared on the bottom right of this scale to warn
pilots of the calculated airspeed at which the stick shaker would activate. The cue’s red color is
consistent with a warning indication requiring immediate recognition and corrective action by
either pilot. The ref speeds switch, when set to increase, adjusts the position of the low-speed cue
to account for the increased stall protection margin.
About 2216:09, the low-speed cue began to rise from the bottom of the airspeed display
as the airspeed slowed. However, the flight crew made no remarks and took no actions that were
consistent with the recognition of this cue. Also, because the autopilot altitude hold mode was
engaged when the airplane leveled off at 2,300 feet, the autopilot continued to add nose-up pitch
trim to maintain altitude as the airspeed slowed. During the time that the low-speed cue was in
view, the airplane’s pitch trim increased from 1° to 7° nose up, and the pitch attitude of the
airplane increased from 3° to 9° nose up. Neither pilot remarked about the increasing pitch
attitude, even though it was a cue indicating that airspeed was slowing. In addition, the numbers
on the airplane’s IAS display changed from white to red as the airplane reached the calculated
stick shaker activation speed. About 2216:27, the stick shaker activated at an airspeed of 131
knots, which was 13 knots higher than the V
ref
that the flight crew had set but 7 knots lower than
the V
ref
icing speed.
It is not unusual for a flight crew to see the low-speed cue appear during an approach
given the airspeed range displayed on the PFDs. When the cue does appear, however, increased
vigilance is necessary to ensure that the airspeed does not slow into the low-speed cue region,
which would result in stick shaker activation. Pilots can accomplish such vigilance by using cues
from the airspeed (actual IAS versus desired IAS), airplane configuration, pitch attitude, and
power, all of which are part of a normal instrument scan. In this accident, the rise of the low-
speed cue toward the decreasing IAS during an 18-second period should have been a salient cue
to elicit action from either pilot. The NTSB concludes that explicit cues associated with the
impending stick shaker onset, including the decreasing margin between indicated airspeed and
the low-speed cue, the airspeed trend vector pointing downward into the low-speed cue, the
changing color of the numbers on the airplane’s IAS display, and the airplane’s excessive nose-
up pitch attitude, were presented on the flight instruments with adequate time for the pilots to
initiate corrective action, but neither pilot responded to the presence of these cues.
2.2.2.1 Possible Reasons for Failed Detection of Impending Stick Shaker
Onset
To identify possible reasons the pilots failed to detect and correct the impending stick
shaker onset, the NTSB examined how the pilots’ attention was directed and what their workload
189
Even though the autopilot had been on throughout most of the flight, power was controlled manually by the
captain because the airplane was not equipped with autothrottles. Both pilots recognized, as a result of their training,
that the airplane did not have an autothrottle system and that power had to be applied manually.

NTSB Aircraft Accident Report
85
had been during the seconds preceding the event. As the flying pilot, the captain should have
been alerted to the rising low-speed cue and should have taken corrective actions during the 18
seconds between the first appearance of the cue and the onset of the stick shaker. Although the
CVR contained statements and actions that were consistent with the captain referencing the
PFD,
190
the NTSB could not precisely determine when he was, or was not, looking at the
airspeed indicator or where else he might have been focusing his attention during this period.
191
As the monitoring pilot, the first officer should have been the primary backup to the
captain and noticed his monitoring error. However, during the time between the first appearance
of the low-speed cue and the onset of the stick shaker, the first officer was performing tasks that
directed her attention toward the center pedestal and the center of the instrument panel and away
from the PFD. About 2216:06, in response to the captain’s “gear down” callout, the first officer
lowered the landing gear and adjusted the condition levers.
192
About 6 seconds later, the first
officer acknowledged a change to the ATCT frequency, and about 3 seconds afterward made a
double chime notification to the flight attendant. About 2216:21, the first officer confirmed that
the gear was down. About 2 seconds later, the captain requested that the flaps be set to 15° and
that the before landing checklist be accomplished. About 5 seconds afterward, and about 1
second before the stick shaker activated, the first officer moved the flap handle to the 10°
position in response to the captain’s callout for flaps 15. (The flap handle had previously been in
the 5° position.)
193
The NTSB concludes that the reason the captain did not recognize the impending onset of
the stick shaker could not be determined from the available evidence but that the first officer’s
tasks at the time the low-speed cue was visible would have likely reduced opportunities for her
timely recognition of the impending event; the failure of both pilots to detect this situation was
the result of a significant breakdown in their monitoring responsibilities and workload
management.
The NTSB also considered the possibility that the pilots were unaware of the effect that
the ref speeds switch position had on the stick shaker activation speed. However, both pilots
were familiar with the airplane’s ice protection system, and the Bombardier Q400 AFM
cautioned that a stall warning might occur if airspeed was not increased before the ref speeds
switch was selected to the increase position. As a result, it is unlikely that the pilots were
unaware of the switch’s effect.
190
These statements included “approach is armed” about 2215:32, “gear down loc’s [localizer is] alive” about
2216:04, and “flaps fifteen before landing checklist” about 2216:24. In addition, a sound similar to a decrease in
engine power was recorded about 2216:00.
191
The captain could have possibly been referencing the approach chart. It is also possible that he was
inspecting the condition of the wings or the ice protection system because an ice detect message appeared on the
engine display about 2216:25. It is important to note that no correlation existed between the timing of the message
and the activation of the stick shaker 2 seconds later.
192
Colgan procedures indicated that these tasks were to be performed by the monitoring pilot.
193
Less than 1 second before the stick shaker activated, the first officer stated, “uhhh.” This statement could
have indicated her recognition of the position of the low-speed cue on the PFD, or it could have been associated
with the start of the before landing checklist. The available information was not sufficient to attribute the meaning
of this statement.
NTSB Aircraft Accident Report
86
The CVR did not record the captain, during the climb to cruise altitude, stating that he
had changed the position of the ref speeds switch from off to increase. However, the CVR did
record the captain and the first officer referring to the 24-hour ice protection check, which
included turning the ref speeds switch to the increase position and then back to the off
position.
194
Also, neither the captain nor the first officer mentioned the status of the switch
during the flight, even with the “INCR REF SPEED” indication that would have appeared on the
engine display.
195
Further, if the ref speeds switch had been turned to the off position after stick
shaker activation, the shaker would have stopped. As a result, the NTSB concludes that the flight
crew did not consider the position of the ref speeds switch when the stick shaker activated.
As indicated in section 1.18.3, after the accident, another Colgan flight crew experienced
the activation of the stick shaker during a night VMC approach to BTV after losing awareness of
the position of the ref speeds switch (which had been set to increase) and failing to recognize the
impending stick shaker onset.
196
The BUF accident, the BTV event, and postaccident interviews
with company pilots demonstrated that Colgan’s approach procedures for setting airspeed bugs
did not reinforce awareness of the ref speeds switch position, which created an opportunity for
confusion. Specifically, pilots were not provided with specified airspeed targets beyond V
ref
, and
no procedures were in place to ensure that the selected airspeeds were above the top of the low-
speed cue. For example, if the captain and the first officer had recalled that the switch was set to
the increase position, then they should have recognized that the airspeed for the approach needed
to increase by 20 knots. Additional information on Colgan’s airspeed selection procedures is
discussed in section 2.8, along with the company’s postaccident changes to these procedures.
2.2.3 Response to Stick Shaker Activation
After the stick shaker activated, the autopilot disconnected automatically, as designed.
The airplane was not in an aerodynamic stall at that time. The stick shaker activated with enough
airspeed available to correct the situation because the wings were level and the load factor was 1
G. However, as stated previously, the captain’s inappropriate aft control column inputs in
response to the stick shaker led to an aerodynamic stall.
CVR and FDR data showed that the captain made an initial aft control column input after
stick shaker onset and before the application of power. The stick forces at the time of autopilot
disconnect were likely less than 2 pounds and would not account for his control input, which was
194
The CVR recorded the captain stating that the 24-hour ice protection check had been accomplished. The
first officer subsequently confirmed that the check had been performed after she noticed in the airplane’s logbooks
that a previous flight crew had not completed the daily check.
195
In addition, if the ref speeds switch was in the off position, the ice detected message on the engine display
would appear in flashing yellow letters, which would have provided the pilots with information about the mismatch
between the position of the ref speeds switch and the airspeed bugs.
196
When the event occurred, the airplane was not under autopilot control. The captain, who was the flying
pilot, reported that she had been looking outside for the runway when the stick shaker activated, and the first officer
reported that he had been performing a checklist at the time. The captain successfully recovered the airplane, and
the flight continued to a landing without further incident.
NTSB Aircraft Accident Report
87
abrupt and inappropriate.
197
The aft control column input occurred within 1 second of the stick
shaker activation, which suggested that the captain’s hands were close to or resting on the
control column. However, it was not possible to determine whether the captain’s hands were
lightly placed on the control wheel before the onset of the stick shaker and the initial aft input
was the result of a rough grab in response to being startled by the activation of the stick
shaker.
198
The aft control column movement was relaxed momentarily, but no evidence showed that
the control column was pushed forward enough to prevent or recover from a stall. (The control
column did not move forward of its neutral position any time after stick shaker activation.)
NTSB postaccident observations in a Q400 flight simulator (with no simulated ice) showed that
Colgan’s recovery procedures after initial stick shaker activation did not require exceptional
piloting skills or aggressive inputs on the flight controls, even when full power was applied
during the recovery effort.
The captain’s subsequent control inputs were also not appropriate because he pulled back
on the column rather than pushed forward to reduce AOA. As a result, the airplane’s pitch
attitude and AOA increased and its airspeed decreased. After the stall, the AOA oscillated
between 10° and 27°, the airspeed remained below the low-speed cue value, and the stick shaker
remained active.
According to Colgan’s procedures for a stall recovery, the captain, as the flying pilot,
was to call “stall,” increase power to the rating detent, and call “check power,” but he did not
follow these procedures. Even though the captain added power in response to the stall warning,
he did not add full power as required.
199
Also, the first officer did not call “stall” when the
captain failed to do so, inform him that power had not been increased to the rating detent (she
would have been able to observe the position of the power levers), or advance the power to the
rating detent when the captain failed to do so. The next steps in the stall recovery procedure
would have been for (1) the first officer, as the monitoring pilot, to call “positive rate” as an
indication that the airplane was climbing; (2) the captain to call “gear up”; (3) the first officer to
raise the gear and call “V
fri
” when the airspeed had accelerated to 125 knots; and (4) the captain
to call for flaps 0.
In addition, the captain had not yet called for the landing gear to be raised or for the flaps
to be retracted. However, about 7 seconds after the stick shaker activated, the first officer raised
the flaps and then told the captain about the action she had just taken. All of Colgan’s procedures
197
The NTSB considered the possibility that the captain’s initial aft input was the result of unrecognized
spatial disorientation. Accelerations and decelerations can be misinterpreted by pilots as pitch cues, which is a
condition known as the somatogravic illusion. However, for this event, the deceleration would not have provided
perceived nose-down pitch cues of sufficient magnitude to explain the captain’s action.
198
To facilitate pilot corrective action in the event of an unexpected autopilot disconnect and minimize the
potential for errant flight as the pilot takes manual control, it is good technique for a pilot to lightly follow along
with the flight controls during approaches flown with the autopilot engaged.
199
FDR data showed that the captain advanced the power levers to about 70°, but the rating detent was 80°.
The rating detent was not a physical stop and required tactile feedback to positively identify its location as the
power levers were advanced. It is possible that the captain missed this feedback as he advanced the throttles.

NTSB Aircraft Accident Report
88
pertaining to flap movement required a command from the flying pilot and acknowledgment
from the monitoring pilot before the flaps could be moved.
The stick pusher activated when the airplane’s airspeed had decreased to about 100 knots
and its AOA was about 18° (which was about 10° higher than the AOA at the time of stick
shaker onset). FDR data showed that the control column moved forward temporarily after stick
pusher activation and then moved aft. The stick pusher activated a second time when the AOA
was about 21° and a third time when the AOA was about 22°, but the control column continued
to remain aft of its neutral position. The NTSB is concerned that the captain pulled against the
stick pusher three separate times during the stall event and that his control inputs fought the stall
protection system’s attempts to decrease the AOA and reduce the severity of the situation.
200
Before transitioning to the Q400, the captain had previously flown the Saab 340, which
had a stick pusher. It is possible that he had seen a demonstration of the stick pusher during
simulator training for that airplane.
201
However, it could not be determined whether the captain
had seen a stick pusher demonstration on the Q400. Even if the captain had seen this
demonstration, his actions in pulling against the pusher were not consistent with any trained
procedure or the basic requirements for recovery from an aerodynamic stall.
If the captain had not overridden the stick pusher’s action to decrease AOA, then the
pusher would have forced the nose of the airplane downward. Also, if the captain would have
responded properly to this nose-down input, then the airplane might have recovered flying speed
in sufficient time to avoid the impact. However, the raising of the flaps, in addition to the vertical
loading at the time, increased the stall speed and reduced the lift being produced by the wings at
a time when the airplane was already stalled.
About 7 seconds after notifying the captain about the status of the flaps, the first officer
asked him whether she should raise the gear, and he consented. The raising of the gear was not
appropriate but had minimal effect on the attempted stall recovery.
In general, the captain’s performance suggests that he was surprised by the stick shaker’s
activation, and he responded by making control inputs that were inappropriate for the situation.
The captain’s failure to make a standard callout or even a declarative statement associated with a
recovery attempt and his failure to silence the autopilot disconnect horn (which continued for the
remainder of the flight and could have been silenced using a button on the control wheel) further
suggest that he was not responding to the situation using a well-learned habit pattern. The first
officer was not providing guidance consistent with an understanding of the situation, suggestions
for corrective input, or standard callouts. In addition, neither flight crewmember made reference
to the airplane’s airspeed at any time after the activation of the stick shaker. During the public
hearing for this accident, the NASA-Ames Research Center chief scientist for aerospace human
factors stated that people under stress might not respond appropriately to events in their
200
Overriding the stick pusher required an 80-pound opposite breakout force and then 66 pounds of continued
aft force. FDR and stall protection system data showed that the stick pusher activated a second time about 2216:40,
and the CVR recorded the captain making a grunting sound about 2216:42.
201
The syllabus for Saab 340 simulator training showed “demonstration to pusher” as an instructor’s discretion
item listed under stalls.
NTSB Aircraft Accident Report
89
environment. In this case, the airplane was in a low-speed, nose-high attitude and was
aerodynamically stalled, and neither pilot responded appropriately to the situation.
The captain’s response to the stick shaker should not have required cognitive effort to
make the correct inputs or standard callouts. Although the conditions under which the captain
had practiced stall recoveries—which should have formed the sequence of actions used in his
response—did not involve an autopilot disconnect or an element of surprise, the captain’s
experience should still have allowed him to quickly adapt to the situation and perform correctly,
as demonstrated by the pilot response during the Colgan BTV event.
202
The accident captain’s history of training failures (previously discussed in section 1.5.1.2
and analyzed in section 2.7) showed that he had demonstrated weaknesses throughout his career
with instrument flying skills and had relied heavily on the autopilot to help him stabilize the
airplane, which might have contributed to his deficient performance during the accident flight.
However, research has shown that it could be difficult for pilots to recognize and recover from
unusual attitudes that were unexpected. In addition, the night and poor visibility conditions at the
time precluded the use of external visual cues for reliable attitude reference, and the airplane’s G
loads and proximity to the ground would have increased the stress associated with the event. The
NTSB concludes that the captain’s response to stick shaker activation should have been
automatic, but his improper flight control inputs were inconsistent with his training and were
instead consistent with startle and confusion. The NTSB further concludes that the captain did
not recognize the stick pusher’s action to decrease AOA as a proper step in a stall recovery, and
his improper flight control inputs to override the stick pusher exacerbated the situation.
2.2.3.1 Possible Reasons for Failed Recovery Procedures
The captain and the first officer had performed approach-to-stall recoveries multiple
times during training at Colgan, with no documented or reported deficiencies. As a result, the
NTSB considered possible reasons for the captain’s and the first officer’s actions during the
attempted recovery.
The NTSB evaluated whether the captain responded incorrectly to the stick shaker onset
because he was applying corrective techniques that would have been more appropriate for a
tailplane stall event. The captain (as well as the first officer) had seen, during initial and
recurrent ground school, a NASA-produced icing video that discussed tailplane stalls and
recovery techniques.
203
The video indicated that tailplane stalls were most likely to occur with
regional and corporate turboprop airplanes
204
and during flight in icing conditions with ice
202
During the BTV event, the captain’s response to the stick shaker was consistent with the company’s stall
recovery procedures. The captain applied forward pressure on the control column and full power. The airspeed
immediately increased, and the stick shaker discontinued.
203
Colgan personnel did not specify the total number of times that the flight crew would have seen the video
during training, but the NTSB estimates that the captain and the first officer would have most likely seen the video
four and two times, respectively.
204
The Q400 was not specifically mentioned as an example of a regional turboprop airplane that was prone to
tailplane stalls; the video was produced before the airplane entered service.

NTSB Aircraft Accident Report
90
present on the horizontal stabilizer. Bombardier, Transport Canada, and the FAA stated during
public hearing testimony that the Q400 was not susceptible to tailplane stalls.
205
In addition,
Colgan had no written procedure for tailplane stalls and did not include tailplane stall training for
the Q400.
The tailplane stall recovery procedure presented in the video called for pulling back on
the control column and reducing flaps, which the accident flight crew did. However, the video
also stated that tailplane icing symptoms were lightening of the controls, pitch excursions,
difficulty in pitch trim, control buffeting, and sudden nose-down pitch, none of which occurred
before the stick shaker activation during the accident flight. Further, the activation of the stick
shaker was a clear warning of an impending conventional aerodynamic stall and not a tailplane
stall, and the change in the IAS numbers to red (which occurred after the airspeed was equal to
or below that of the low-speed cue) was a conspicuous signal that was not consistent with a
tailplane stall. Also, indications of a tailplane stall, for those airplanes determined to be
susceptible, would likely occur at higher airspeeds and/or higher flap deflections.
For a tailplane stall recovery, the captain would have had to interpret the situation,
identify the tailplane stall, and apply a recovery procedure that he had never practiced. The CVR
showed that he did not verbally identify a tailplane stall, and the FDR showed that he did not
fully apply the tailplane stall recovery procedure described in the video. The NTSB concludes
that it is unlikely that the captain was deliberately attempting to perform a tailplane stall
recovery. The NTSB further concludes that no evidence indicated that the Q400 was susceptible
to a tailplane stall. (Tailplane stall training is discussed further in section 2.9.3.)
The NTSB also evaluated why the first officer had raised the flaps without being so
directed by the captain. The stick shaker activated within 1 second of the first officer moving the
flap handle from 5° to 10°. It is possible that, because of the close timing of these events, the first
officer’s retraction of the flaps was an attempt to undo her last action. However, after returning
the handle to the 5° position, the first officer continued moving the handle to the 0° position.
206
It is also possible that she misinterpreted the event as a tailplane stall, and retracting the flaps to
the last position before a tailplane stall was a recommended technique that she had been exposed
to while watching the NASA icing video during recurrent ground school less than 1 month
before the accident. Also, the absence of standard callouts from the captain impeded the first
officer’s abilities to coordinate actions to support him. Further, it is possible that she raised the
flaps as part of the steps associated with a landing stall recovery profile. However, if that were
the case, the first officer failed to make the “positive rate” or “V
fri
” callouts or confirm that
power was set, which were required before raising the flaps. Finally, it is possible that the first
officer raised the flaps because she had reverted to her previous general aviation experience; as a
certified flight instructor, stall recoveries were not crew-coordinated maneuvers, and the flying
pilot raised the flaps incrementally during th
207
e recovery.
205
The testing that was performed to make this determination is described in section 1.17.1.2.
206
Although each flap handle position has a detent, it is possible to traverse a particular detent quickly (in
about 1 second). The FDR flap handle position parameter is sampled every 2 seconds, so the actual time between
the positioning of the flap handle in the detents for 5° and 0° is not known.
207
Section 1.5.2.2 describes the first officer’s previous approach-to-stall training.

NTSB Aircraft Accident Report
91
In addition, the NTSB evaluated why the first officer suggested raising the landing gear.
Her suggestion could have been in response to the ambiguous statement made by the captain
following his grunting sound about 2216:42 (*ther bear).
208
However, her suggestion occurred
about 4 seconds later and not immediately afterward. Another possibility is that the first officer
was attempting to provide support to the captain because raising the gear is one of the steps in
the stall recovery procedure, but the “gear up” callout was the responsibility of the flying pilot,
and the steps that preceded that callout had not been accomplished.
The NTSB concludes that, although the reasons the first officer retracted the flaps and
suggested raising the gear could not be determined from the available information, these actions
were inconsistent with company stall recovery procedures and training.
2.2.4 Captain’s Management of Flight
The captain was responsible for the management of the flight. However, he and the first
officer engaged in conversations for much of the flight,
209
starting about 6 minutes 40 seconds
after takeoff as the airplane was climbing to 12,000 feet during the ascent to its cruise altitude.
(The airplane had reached an altitude of 10,000 feet about 2 minutes before the conversations
began.) Although the conversations during cruise flight did not conflict with Federal regulations
or company policy, their depth and duration likely contributed to the delayed performance of
callouts and checklists.
210
For example, Colgan’s Q400 CFM indicated that the cruise checklist
should be performed after the airplane attained its assigned cruising altitude,
211
as the flying
pilot leveled the airplane and allowed it to accelerate to the maximum operating limit speed
minus 10 knots. However, the captain called for the cruise checklist about 2138:47, which was
about 2.5 minutes after the airplane had accelerated to cruise speed.
The airplane began descending from its 16,000-foot cruise altitude about 2157:20.
Although Colgan’s Flight Operations Policies and Procedures Manual stated that approach
briefings should generally be accomplished before the top of the descent (when the crew’s
workload was expected to be minimal), the captain did not start this briefing until 2204:16, as the
airplane descended below 12,000 feet.
212
The manual also required a callout by the flying pilot
when the airplane was descending through 10,000 feet, but the captain was conducting the
approach briefing at that time and omitted the callout.
208
The asterisk denotes an unintelligible word.
209
Between the time that the airplane left the gate at EWR and the time that it was cleared for takeoff, 1 hour
33 minutes had elapsed. During the ground time at EWR that was captured by the CVR, the flight crew engaged in
lengthy conversations that were not directly related to the operation, which set the tone for the flight.
210
The captain was also late with a checklist callout earlier in the flight. Colgan’s Q400 CFM indicated that the
taxi checklist should begin after an airplane leaves the ramp area. However, the captain called for the checklist
about 2115:51, which was 45 minutes after the airplane left the ramp area.
211
The 24-hour ice protection check was performed as part of the cruise checklist.
212
The captain conducted a complete and accurate approach briefing in accordance with Colgan procedures
with the exception of one briefing item. A flight data center notice to airmen had been issued to modify the ILS
runway 23 missed approach procedure. Even though the captain should have briefed this information, the flight
crew would have received instructions from ATC for the missed approach procedure.

NTSB Aircraft Accident Report
92
Once the airplane had descended through 10,000 feet (about 2206:37), sterile cockpit
procedures, prohibiting nonpertinent conversations within the cockpit, were required. However,
the flight crewmembers engaged in a nonpertinent conversation during the final minutes of the
descent, which distracted them from their flying duties.
213
About 2210:23, the first officer asked whether ice was present on the windshield. After a
brief exchange between the pilots as they inspected the ice, the captain stated that it was the most
ice he had seen on the leading edges in a long time. About 2210:58, the first officer initiated a
nonpertinent conversation about her experience flying in icing conditions. The captain
participated in this conversation, which continued for a period of about 80 seconds, until it was
interrupted by an ATC clearance to descend to 2,300 feet. About 2212:33, after the pilots
confirmed the altitude entry in the autopilot and had a brief discussion about the autopilot mode,
they resumed their conversation until ATC called 11 seconds later with a heading instruction.
About 2213:01, the captain and the first officer again resumed the conversation for
another 15 seconds until the altitude alerter sounded to indicate that the airplane was descending
through 3,300 feet. At that point, the captain called for the descent checklist, but Colgan’s Q400
CFM stated that the descent checklist was to begin at the top of the descent if the cruise altitude
was below 18,000 feet. The captain called for the approach checklist about 11 seconds later,
immediately after completion of the descent checklist. However, the CFM stated that this
checklist was to be completed before an airplane on an instrument approach transitioned to the
initial approach phase, but the accident airplane was at a point inside the initial approach fix at
the time of the captain’s callout. After the descent and approach checklists were completed, the
first officer resumed the conversation until about 2214:09, when another ATC call was received.
The pilots were responsible for performing operational tasks during their 3-minute 11-
second nonpertinent conversation. In addition, the conversation followed the first officer’s
identification of a possible threat to the airplane (ice), but neither pilot took appropriate actions,
such as confirming the ice protection system’s status or the airspeed targets, to ensure that the
threat was mitigated.
As previously stated in section 2.2.2, the captain had the primary responsibility to
monitor the instruments, and the first officer was responsible for providing backup to the
captain. However, as part of his overall workload management responsibilities, the captain
should have been cognizant of the tasks that he requested the first officer to perform and their
effect on her ability to reliably provide the expected monitoring and cross-check. As a result, he
should have been especially focused on the flight instruments during these periods. However, he
did not notice the rising low-speed cue on the IAS display (especially during the 18 seconds
before stick shaker activation, when the first officer would have been configuring the airplane
for landing), even though the pilots’ nonpertinent conversation had ended about 2 minutes before
the appearance of the low-speed cue.
213
About 2207:22, the first officer made the “in-range” call to Colgan operations at BUF. However, according
to the company’s Flight Operations Policies and Procedures Manual, this call should have been made before leaving
cruise flight.

NTSB Aircraft Accident Report
93
Because of their conversation, the flight crewmembers squandered time and their
attention, which were limited resources that should have been used for attending to operational
tasks, monitoring, maintaining situational awareness, managing possible threats, and preventing
potential errors. As a result, the NTSB concludes that the captain’s failure to effectively manage
the flight (1) enabled conversation that delayed checklist completion and conflicted with sterile
cockpit procedures and (2) created an environment that impeded timely error detection.
Additional information on captain leadership and sterile cockpit procedures appears in sections
2.4.1 and 2.4.2, respectively.
2.3 Strategies to Prevent Monitoring Failures
The flight crewmembers failed to monitor the airplane’s pitch attitude, power, and
especially its airspeed and failed to notice, as part of their monitoring responsibilities, the rising
low-speed cue on the IAS display. Multiple strategies can be used to protect against catastrophic
outcomes resulting from these and other monitoring failures, including flight crew training, flight
deck procedures, and low-airspeed alert systems, which are discussed in sections 2.3.1 through
2.3.3, respectively.
2.3.1 Flight Crew Monitoring Training
The NTSB has long recognized the importance of flight crew monitoring skills in
accident prevention. In its 1994 safety study of 37 flight crew-involved major accidents, the
NTSB found that, for 31 of these accidents, inadequate monitoring and/or cross-checking had
occurred.
214
The study also found that flight crewmembers frequently failed to recognize and
effectively draw attention to critical cues that led to the accident sequence, which was further
demonstrated by the circumstances of this accident.
As part of its safety study, the NTSB issued Safety Recommendations A-94-3 and -4 to
the FAA concerning the need for enhanced training of pilot monitoring skills. The
recommendations stated, in part, that the FAA should require Part 121 air carriers to provide line
operational simulation training that “allows flightcrews to practice, under realistic conditions,
non-flying pilot functions, including monitoring and challenging errors made by other
crewmembers” and that the carriers’ IOE should include training and experience for check
airmen and pilots “in enhancing the monitoring and challenging functions.” On January 16,
1996, the NTSB classified these recommendations “Closed—Acceptable Alternate Action”
based on the FAA’s revised training guidance (AC 120-51B), which emphasized the importance
of monitoring.
Another accident involving monitoring failures occurred in February 2005 when a
Cessna Citation crashed on approach to Pueblo, Colorado. In its report on the accident (see
214
For additional information, see National Transportation Safety Board, A Review of Flightcrew-Involved,
Major Accidents of U.S. Carriers, 1978 through 1990, Safety Study NTSB/SS-94/01 (Washington, DC: NTSB,
1994).

NTSB Aircraft Accident Report
94
section 1.18.1.4), the NTSB cited the flight crew’s “failure to effectively monitor and maintain
airspeed” as part of the probable cause and issued Safety Recommendation A-07-13, which
asked the FAA to do the following:
Require that all pilot training programs be modified to contain modules that teach
and emphasize monitoring skills and workload management and include
opportunities to practice and demonstrate proficiency in these areas.
On May 17, 2007, the FAA stated that it would consider identifying, in its work program,
a list of required inspections that would reemphasize, to regional office and FSDO managers, the
need to validate the training that was already required and verify its effectiveness. On September
10, 2008, the NTSB stated that such a list would be responsive to the intent of the
recommendation as long as the list provided a strong emphasis on the monitoring and workload
management components of a CRM program. The NTSB classified the recommendation
“Open—Acceptable Response.”
The importance of monitoring was referenced in some of Colgan’s guidance to its
pilots
215
and was discussed and evaluated during simulator training and IOE. However, the
company did not provide specific pilot training that emphasized the monitoring function.
Further, the company’s CRM training did not explicitly address monitoring or provide pilots
with techniques and training for improving their monitoring skills.
216
During public hearing testimony, the NASA-Ames Research Center chief scientist for
aerospace human factors stated that people have limited attention and must select from among
those features in their environment to direct their attention. Also, distractions and interruptions
can increase workload and redirect attention, thus complicating the monitoring task. As a result,
effective monitoring requires active effort.
To improve monitoring skills, pilots must proactively seek information and ask questions.
The NASA chief scientist testified that current pilot training programs do not typically train
these skills in a systematic manner. The NTSB concludes that the monitoring errors made by the
accident flight crew demonstrate the continuing need for specific pilot training on active
monitoring skills. Almost 3 years have passed since Safety Recommendation A-07-13 was
issued, and more than 2.5 years have passed since the FAA described to the NTSB the planned
actions to address the recommendation. Since that time, the FAA has reported no further action
on this recommendation, even after receiving the NTSB’s September 2008 response letter.
Therefore, the NTSB reiterates Safety Recommendation A-07-13 and reclassifies it “Open—
Unacceptable Response.”
215
The CFM made only minimal reference to the responsibilities of the monitoring pilot during approach
profiles.
216
The company’s current training for CRM/threat and error management presents information on the
importance of monitoring as a strategy to detect and prevent errors.
NTSB Aircraft Accident Report
95
2.3.2 Flight Deck Procedures
The FAA has developed guidance on the design of procedures to facilitate pilot
monitoring and cross-checking. These procedures are contained in an appendix to AC 120-71A,
“Standard Operating Procedures for Flight Deck Crewmembers.” The guidance provides
examples of and supporting rationale for standard operating procedures that promote monitoring.
The guidance also recommends establishing standard operating procedures to support improved
monitoring during climb, descent, and approach.
Colgan’s standard operating procedures did not include speed targets during approaches;
these targets would have facilitated the detection of speed deviations by the monitoring pilot.
Colgan also lacked standardized procedures for setting airspeeds and using the ref speeds switch,
which did not promote effective cross-checking between airspeeds and the switch’s status.
(These issues are discussed in section 2.8.) If such procedures had been in place, then the flight
crew might have detected the inconsistency between the 118-knot V
ref
(a non-icing speed) and
the position of the ref speeds switch (icing conditions assumed) and ensured that a V
ref
of 138
knots (an icing speed) was selected. Further, although company procedures required the flying
pilot to make a 1,000-foot callout when changing altitudes, the director of flight standards stated
that the callout was not required before the altitude alerter sounded. Such a practice can impede
monitoring because flight crews may become passive and wait for an automated backup system
to prompt their required callout.
217
After the accident, the company introduced the “VVM”
(verbalize, verify, and monitor) program to improve flight crew monitoring.
218
The NTSB concludes that Colgan Air’s standard operating procedures at the time of the
accident did not promote effective monitoring behavior. The NTSB is concerned that other air
carriers’ standard operating procedures may also be deficient in this area. Therefore, the NTSB
recommends that the FAA require Part 121, 135, and 91K
219
operators to review their standard
operating procedures to verify that they are consistent with the flight crew monitoring techniques
described in AC 120-71A; if the procedures are found not to be consistent, revise the procedures
according to the AC guidance to promote effective monitoring.
2.3.3 Low-Airspeed Alert Systems
The low-speed cue and the stick shaker on the Q400 were intended to warn the pilots of
an impending stall. In this case, even though both systems functioned as designed, neither pilot
responded appropriately to prevent the stall. Features on the airspeed display, including the
indicated airspeed, trend vector, and low-speed cue, should have provided the pilots with
adequate time to detect the rising low-speed cue and respond appropriately. However, distraction
217
This practice, known as primary backup reversion, is characterized by a human operator using an automated
backup system as the primary signal to be monitored.
218
Colgan also discussed the importance of monitoring in its revised CRM/threat and error management
course. Also, the company’s revised Flight Operations Policies and Procedures Manual reinforced this training by
stating that all pilots were expected to “actively demonstrate monitoring and challenging” as a CRM skill during
line operations.
219
Title 14 CFR 91 Subpart K applies to fractional ownership operations.

NTSB Aircraft Accident Report
96
and workload considerations may have made it difficult for the pilots to visually detect features
on the airspeed display depicting the development of this condition (including the trend vector
and the low-speed cue), so a redundant aural alert might have provided them with an effective
warning about the decreasing airspeed in relation to the rising position of the low-speed cue.
In its report on the October 2002 King Air A100 accident in Eveleth, Minnesota, the
NTSB found that the pilots had allowed the airspeed to decrease to dangerously low levels while
attempting to execute a nonprecision instrument approach during instrument meteorological
conditions. As a result, the airplane entered an aerodynamic stall from which the flight crew did
not recover. Because the flight crew failed to recognize that the stall was imminent, the NTSB
concluded that the development of and requirement for the installation of a low-airspeed alert
system could substantially reduce the number of accidents and incidents involving a flight
crew’s failure to maintain airspeed.
On December 2, 2003 the NTSB issued Safety Recommendations A-03-53 and -54,
which asked the FAA to do the following:
Convene a panel of aircraft design, aviation operations, and aviation human
factors specialists, including representatives from the National Aeronautics and
Space Administration, to determine whether a requirement for the installation of
low-airspeed alert systems in airplanes engaged in commercial operations under
14 Code of Federal Regulations Parts 121 and 135 would be feasible, and submit
a report of the panel’s findings. (A-03-53)
If the panel requested in Safety Recommendation A-03-53 determines that a
requirement for the installation of low-airspeed alert systems in airplanes engaged
in commercial operations under 14 Code of Federal Regulations Parts 121 and
135 is feasible, establish requirements for low-airspeed alert systems, based on
the findings of this panel. (A-03-54)
On October 3, 2006, the FAA stated that it had formed a team to assess the feasibility of
low-airspeed alert systems. On April 3, 2007, the NTSB stated it was encouraged that the FAA
had formed the team and would begin addressing the recommendation. As a result, the
recommendation was classified “Open—Acceptable Response.”
During the almost 6 years since the NTSB issued Safety Recommendations A-03-53 and
-54, (which were reiterated in July 2006 after another event involving decreasing airspeed and
loss of control),
220
accidents and incidents involving a lack of flight crew awareness of
decreasing airspeed have continued, indicating that existing stall warnings are not a reliable
method for preventing inadvertent hazardous low-speed conditions. The NTSB notes that human
220
The recommendations were reiterated in a safety recommendation letter addressing an incident involving
American Eagle flight 3008, a Saab 340 airplane that experienced a loss of control during icing conditions. The
letter also addressed three similar Saab 340 incidents investigated by the Australian Transport Safety Bureau and
stated, “if the flight crews had been alerted to the rapid airspeed decrease in a timely fashion, they may have been
able to take corrective action and perhaps avoid the stall.”
NTSB Aircraft Accident Report
97
factors concerns associated with a low-airspeed alert do not require more than 6 years of study
for a solution to be implemented.
221
The NTSB notes that several other airplanes certificated under 14 CFR Part 25, including
the Boeing 747-400 and 777, provide pilots with an amber band on the airspeed display above
the low-speed cue. This amber band typically represents the airspeed between the stall warning
speed and the minimum maneuvering speed. Operations are not normally conducted with
airspeeds in the amber band, which, in effect, provides pilots with a visual indication of a
developing low-speed condition before the onset of the stall warning.
AC 25-11A, “Electronic Flight Displays,” discusses the visual design of low-speed
awareness cues and states, “the preferred colors to be used are amber or yellow to indicate that
the airspeed has decreased below a reference speed that provides adequate maneuver margin,
changing to red at the stall warning speed. The speeds at which the low speed awareness bands
should start should be chosen as appropriate to the airplane configuration and operational flight
regime. For example, low speed awareness cues for approach and landing should be shown
starting at V
ref
with a tolerance of +0 and -5 knots.”
The NTSB concludes that the Q400 airspeed indicator lacked low-speed awareness
features, such as an amber band above the low-speed cue or airspeed indications that changed to
amber as speed decrease toward the low-speed cue, which would have facilitated the flight
crew’s detection of the developing low-speed situation. Therefore, the NTSB recommends that
the FAA require that airspeed indicator display systems on all aircraft certified under 14 CFR
Part 25 and equipped with electronic flight instrument systems depict a yellow/amber cautionary
band above the low-speed cue or airspeed indicator digits that change from white to
yellow/amber as the airspeed approaches the low-speed cue, consistent with AC 25-11A,
“Electronic Flight Displays.”
At the public hearing for this accident, an FAA certification specialist testified that
current certification rules under 14 CFR 25.1329 indicate that there should be speed protection
and/or alerting within the normal speed range while under flight guidance system (autopilot)
control. The certification specialist stated, “there should be low speed alerting occurring prior to
stall warning, if you’re under flight guidance system or autopilot control. And that low speed
alerting can take many forms, but it needs to be aural and visual.”
222
On July 9, 2009, the FAA issued an NPRM for flight crew alerting, which included a
requirement that alerts necessitating immediate crew awareness be presented using two sensory
modalities. For example, a visual alert accompanied by an aural alert can help to capture and
221
After the March 19, 2001, incident involving Comair flight 5054, a low-airspeed alert system was
developed for Embraer EMB-120 airplanes. The system was designed to provide pilots with an aural and a visual
alert of low airspeed while operating in icing conditions. FAA Airworthiness Directive 2001-20-17, effective
October 22, 2001, mandated installation of the system on the EMB-120.
222
The Q400 was certificated before the amendment to Section 25.1329. AC 25.1329-1B, “Approval of Flight
Guidance Systems,” states, “standard stall warning and high-speed alerts are not always timely enough for the flight
crew to intervene to prevent unacceptable speed excursions during FGS [flight guidance system] operation.” The
AC also states, “a low speed alert and a transition to the speed protection mode at approximately 1.13 Vsr for the
landing flap configuration has been found to be acceptable.” In addition, the AC states, “low speed protection alerts
should include both an aural and visual component.”

NTSB Aircraft Accident Report
focus a pilot’s attention in the event that the pilot is not looking at the alerting cue. In this
accident, the pilots did not likely see the rising low-speed cue on the IAS display, the downward-
pointing trend vector, or the airspeed indications change to red. As a result, the NTSB concludes
that an aural warning in advance of the stick shaker would have provided a redundant cue of the
visual indication of the rising low-speed cue and might have elicited a timely response from the
pilots before the onset of the stick shaker. Therefore, the NTSB recommends that, for all
airplanes engaged in commercial operations under 14 CFR Parts 121, 135, and 91K, the FAA
require the installation of low-airspeed alert systems that provide pilots with redundant aural and
visual warnings of an impending hazardous low-speed condition. Because of the FAA’s
inactivity with regard to Safety Recommendations A-03-53 and -54, the NTSB classifies the
recommendations “Closed—Unacceptable Action/Superseded” and classifies Safety
Recommendation A-10-12 “Open—Unacceptable Response.”
2.4 Pilot Professionalism
2.4.1 Leadership Training
The captain was responsible for setting the appropriate tone in the cockpit and managing
communications and workload in a manner that promoted professionalism and adherence to
standard operating procedures. On the basis of his actions during the flight, including the late
performance of checklists and callouts because of an ongoing conversation, the captain showed
inadequate leadership. His failure to establish the appropriate cockpit tone during the initial
stages of the operation and show strong command authority during the flight is disconcerting,
especially because he had been a captain for more than 2 years.
In March 1998, the FAA mandated CRM training for all Part 121 operators. CRM
training helps facilitate effective crew communication and coordination and the use of available
resources to protect against error. The concepts associated with CRM training have been
expanded to include techniques for threat and error detection, management, and mitigation.
Many operators integrate CRM concepts in their training programs and evaluate CRM skills
during simulator training and line observations. Colgan’s CRM training included 5 slides (of 45
slides total) that addressed command, leadership, and leadership styles. (Colgan’s CRM training
is further discussed in section 2.4.3.)
In contrast, Part 121 operators are not required to provide upgrading captains with
specific training on the leadership skills necessary to make the transition from SIC to PIC. For
many new captains, including the accident captain, the initial upgrade represents the first time in
which they are held responsible for leading and managing multiple crewmembers during air
carrier operations. Because of the PIC’s critical role in establishing and maintaining safe
operating conditions, upgrading captains would greatly benefit from specific training on
command and leadership skills.
The captain upgraded in October 2007; at that time, Colgan provided to its upgrading
captains a 1-day training course on duties and responsibilities. Although the director of
98

NTSB Aircraft Accident Report
99
crewmember and dispatcher training stated that the course was designed to help a new captain
make the transition to the new role, the NTSB’s review of the course content showed that it
focused on the administrative duties associated with becoming a captain. The upgrade training
course did not contain significant content applicable to developing leadership skills, management
oversight, and command authority.
Some air carriers provide leadership training to their upgrading captains. For example,
one regional air carrier expanded its leadership training, from 2 to 8 hours, so that additional
information on leadership skills could be presented. This change was made in response to an
unacceptable level of training failures (primarily because of leadership and judgment factors) for
upgrading captains.
223
The expanded course contained modules on leadership, authority, and
responsibility; briefing and debriefing scenarios; decision-making processes, including those
during an emergency; dry-run line-oriented flight scenarios; and risk management and resource
utilization.
Industry changes (including two-pilot cockpits and the advent of regional carriers) have
resulted in opportunities for pilots to upgrade to captain without having accumulated significant
experience as a first officer in a Part 121 operation. Without these important opportunities for
mentoring and observational learning, which characterize time spent in journeyman pilot
positions, it may be difficult for a pilot to acquire effective leadership skills to manage a
multicrew airplane. In addition, airlines must instill their leadership values and safety culture in
their captains because they are the ones who are ultimately responsible for the safety of each
flight.
At the public hearing for this accident, ALPA’s safety committee chairman discussed the
need for companies to provide leadership skills to upgrading captains and for captains to set the
proper tone in the cockpit. The POI for Colgan stated, during a postaccident interview, that
training in this area was important and should be required.
The NTSB concludes that specific leadership training for upgrading captains would help
standardize and reinforce the critical command authority skills needed by a PIC during air carrier
operations. Some operators are already providing this training, but others are not. Therefore, the
NTSB recommends that the FAA issue an AC with guidance on leadership training for
upgrading captains at Part 121, 135, and 91K operators, including methods and techniques for
effective leadership; professional standards of conduct; strategies for briefing and debriefing;
reinforcement and correction skills; and other knowledge, skills, and abilities that are critical for
air carrier operations. The NTSB further recommends that the FAA require all Part 121, 135, and
91K operators to provide a specific course on leadership training to their upgrading captains that
is consistent with the AC requested in Safety Recommendation A-10-13.
223
The company’s captain upgrade first-time failure rate had reached 22 percent when the target was 10
percent. The company’s POI stated that the failures had involved “captain thinking skills” and not “stick and rudder
skills.” For more information, see the NTSB’s report on the Pinnacle Airlines flight 3701 accident (referenced in
section 1.18.1.3).

NTSB Aircraft Accident Report
100
2.4.2 Sterile Cockpit and Standard Operating Procedures
The pilots were involved in nonpertinent conversation during all phases of flight,
including those that are defined as critical by the sterile cockpit rule. For example, the pilots’
nonpertinent conversation during the final minutes of the descent (which included a discussion
of their previous experiences flying in icing conditions) distracted them from their operational
tasks. In addition, the pilots deviated from standard operating procedures with the timing of
checklists during the descent (as previously discussed in section 2.2.4).
Colgan expected sterile cockpit procedures to be included in a captain’s briefing and
adhered to during training, checkrides, and line operations. Most company pilots interviewed
after the accident stated that sterile cockpit adherence was good and that pilots deviated rarely
from sterile cockpit procedures. Company and FAA oversight before the accident did not
identify any problems with sterile cockpit adherence, but some deviations were identified after
the accident.
Colgan stated that it had provided pilots with information on sterile cockpit procedures
during ground school indoctrination training, but a review of all slides presented during the
training at the time of the accident found none that specifically addressed sterile cockpit
procedures. After the accident, the company revised its training program, and recurrent training
now addresses the importance of sterile cockpit procedures. Also, the company’s chief pilot
issued guidance on sterile cockpit adherence, including a reminder that no extraneous
conversation of any kind could take place when sterile cockpit procedures were in effect.
224
The NTSB is concerned that, during the accident flight, neither pilot seemed hesitant to
engage in nonpertinent conversation or demonstrated correcting behavior when the other pilot
deviated from sterile cockpit procedures. These facts suggest that nonpertinent conversation
among company pilots during critical phases of flight was not unusual.
The primary reason for 14 CFR 121.542, otherwise known as the sterile cockpit rule, is to
ensure that a pilot’s attention is directed to operational concerns during critical phases of flight
and is not redirected or degraded because of nonessential activities or conversation. The NTSB
has investigated accidents demonstrating the catastrophic effects of pilot deviations from
Section 121.542 and standard operating procedures. For example, in August 2006, the flight
crew of Comair flight 5191 attempted to depart from the wrong runway, which resulted in an
accident that killed 49 of the 50 people on board. The NTSB determined that the flight crew’s
nonpertinent conversation during taxi, which resulted in a loss of positional awareness, was a
contributing factor to the accident. The NTSB also found that the flight crew’s noncompliance
with standard operating procedures had most likely created an atmosphere in the cockpit that
enabled the crew’s errors.
225
Nonpertinent conversation during a critical phase of flight and
224
In addition to these changes, Colgan incorporated a discussion of accidents and incidents involving sterile
cockpit breakdowns to its CRM/threat and error management training. Also, Colgan procedures contained an
expanded definition of sterile cockpit periods, including ± 1,000 feet of level-off altitude when making altitude
changes and when approaching the top of descent on crossing restrictions and pilot-discretion descents.
225
For more information, see Attempted Takeoff From Wrong Runway, Comair Flight 5191, Bombardier
CL-600-2B19, N431CA, Lexington, Kentucky, August 27, 2006, Aircraft Accident Report NTSB/AAR-07-05
(Washington, DC: NTSB, 2007).
NTSB Aircraft Accident Report
101
noncompliance with standard operating procedures were also issues found during the
investigation of the Colgan accident.
Other recent accidents have identified similar issues involving a breakdown in cockpit
discipline and noncompliance with the sterile cockpit rule.
226
Although it is difficult to identify a
specific reason for this behavior, industry data have shown that pilots who had intentionally
deviated from standard operating procedures were three times more likely to make other types of
errors, mismanage more errors, and find themselves in more undesirable situations compared
with those flight crewmembers who had not intentionally deviated from procedures.
227
Nevertheless, most airline and FAA personnel have stated, after accidents, that no precursors to
such deviations were identified during their previous oversight activities. The Q400 APM for
Colgan acknowledged that an inspector’s observations of flight crew performance might not be
representative of the crew’s usual performance.
On February 7, 2006, the NTSB issued Safety Recommendation A-06-7, which asked the
FAA to direct the POIs of all Part 121 and 135 operators to reemphasize the importance of strict
compliance with the sterile cockpit rule. In response to this recommendation, the FAA issued
SAFO 06004 on April 28, 2006, to emphasize the importance of sterile cockpit discipline. As a
result of the FAA’s action, the NTSB classified Safety Recommendation A-06-7 “Closed—
Acceptable Action” on November 9, 2006. However, the lasting effect of this SAFO is
questionable given that the Comair flight 5191 accident occurred only 4 months after the SAFO
was issued and the Colgan accident happened less than 3 years after the SAFO’s issuance.
At the public hearing for this accident, an FAA manager stated that the agency has been
addressing sterile cockpit issues through, among other actions, published guidance and oversight
activities by inspection personnel.
228
The NTSB identified only one FAA AC or handbook—the
Instrument Procedures Handbook (FAA-H-8261-1A)—that references an accident involving the
lack of sterile cockpit discipline.
229
In addition, this publication does not include information
that outlines the origin of the sterile cockpit rule, its rationale, and an explicit discussion of the
safety consequences associated with the failure to adhere to sterile cockpit procedures during
critical phases of flight.
226
These accidents include the Corporate Airlines flight 5966 accident (see section 1.18.1.1) and the Pinnacle
Airlines flight 3701 accident (see section 1.18.1.3).
227
These data are from the LOSA Collaborative, which is a network of researchers, safety professionals, pilots,
and airline representatives who collaborate to provide, among other things, oversight and implementation of LOSA
and a forum for information exchange regarding LOSA. Deviations from sterile cockpit procedures are among the
types of intentional noncompliance that can be detected through LOSA observations. In January 2007, the NTSB
issued Safety Recommendation A-07-9 to require Part 121 operators to incorporate LOSA observations into their
oversight programs. This recommendation and its status are discussed in section 1.18.1.9. Colgan has begun to
implement a LOSA program, as discussed in section 1.17.7.4.
228
These publications include AC 120-71A, “Standard Operating Procedures for Flight Deck Crewmembers”;
AC 120-74A, “Parts 91, 121, 125, and 135 Flightcrew Procedures During Taxi Operations”; AC 120-51E, “Crew
Resource Management Training”; and AC 91-73A, “Part 91 and Part 135 Single-Pilot Procedures During Taxi
Operations.”
229
The handbook references the September 1974 Eastern Air Lines flight 212 accident, which was caused by
the flight crew’s lack of altitude awareness at critical points during the approach as a result of poor cockpit
discipline. For more information, see National Transportation Safety Board, Eastern Air Lines, Inc., Douglas
DC-9-31, N8984E, Charlotte, North Carolina, September 11, 1974, Aircraft Accident Report NTSB/AAR-75/09
(Washington, DC: NTSB, 1975).

NTSB Aircraft Accident Report
102
Also at the public hearing, the Colgan director of flight standards testified that
postaccident observations of company pilots revealed only “minor” sterile cockpit deviations,
such as an individual pilot remark about something either heard on the radio or seen. The flight
standards director stated that, in such instances, the other pilot would not respond to the
comment. However, the NTSB recognizes that any nonpertinent remark during critical phases of
flight has the potential to be distracting. Multiple opportunities exist during noncritical phases of
flight to allow flight crewmembers to communicate, establish trust, and build rapport, but, during
critical phases of flight, all conversations need to relate solely to the operation of the flight.
These conversations should follow standard operating procedures and include the use of standard
phraseology, which are proven tools for safely operating aircraft.
Even though the responsibility for sterile cockpit adherence is ultimately a matter of a
pilot’s own professional integrity, the NTSB notes that pilots work within a context of
professionalism created through the mutual efforts of the FAA, operators, and pilot groups.
These stakeholders need to work together to provide clear and unwavering guidance that helps to
instill sound principles of professionalism and adherence to standard operating and sterile
cockpit procedures. The stakeholders also need to provide detailed guidance on these topics to
new commercial pilots as well as instruction and reinforcement on the topics to pilots throughout
their career.
On January 23, 2007, the NTSB issued Safety Recommendation A-07-8, which asked the
FAA to do the following:
Work with pilot associations to develop a specific program of education for air
carrier pilots that addresses professional standards and their role in ensuring
safety of flight. The program should include associated guidance information and
references to recent accidents involving pilots acting unprofessionally or not
following standard operating procedures.
On April 13, 2007, the FAA stated that it would meet with ALPA, the Air Transport
Association, the Regional Airline Association, and other groups to determine an effective
approach for addressing these issues. On January 22, 2008, the NTSB stated that the FAA’s
planned action would be appropriate after the development of an educational program that
conveyed the necessary safety information and classified the recommendation “Open—
Acceptable Response.” However, in the 3 years since the issuance of Safety Recommendation A-
07-8, the FAA has not produced guidance material or developed a program that meets the intent
of the recommendation.
230
The NTSB recognizes that most pilots strive to fly professionally and adhere to standard
operating and sterile cockpit procedures. However, the continuing failure of some pilots to
230
In contrast, the FAA has created instructional materials on other aviation safety-related issues. For example,
to address the increasing problem of runway incursions, the FAA distributed to all pilots a multimedia presentation
and printed guidance on the issue. The presentation addressed runway safety, discussed accidents and operating
rules, and offered best practices and techniques. Such an approach could be effective in addressing breakdowns in
pilot professionalism and sterile cockpit discipline, especially if examples of accidents are included with standard
operating procedures and best practices to help focus attention on the reasons for the standards and the potential
results of not following them.
NTSB Aircraft Accident Report
103
refrain from nonpertinent conversation during critical phases of flight erodes proven margins of
safety provided by the strict adherence to standard operating procedures, as demonstrated by the
circumstances of this accident.
More than 28 years have elapsed since sterile cockpit rulemaking was enacted based on
the NTSB’s investigation of the Eastern Air Lines accident and the professional conduct
recommendations that resulted from the investigation.
231
However, industry action is still needed
to provide all pilots with guidance discussing (1) the importance of following standard operating
procedures, adhering to sterile cockpit procedures, and maintaining professionalism during
aircraft operations and (2) the costs to safety when pilots do not operate according to these
standards.
The NTSB concludes that, because of the continuing number of accidents involving a
breakdown in sterile cockpit discipline, collaborative action by the FAA and the aviation
industry to promptly address this issue is warranted. Therefore, the NTSB recommends that the
FAA (1) develop, and distribute to all pilots, multimedia guidance materials on professionalism
in aircraft operations that contain standards of performance for professionalism; best practices
for sterile cockpit adherence; techniques for assessing and correcting pilot deviations; examples
and scenarios; and a detailed review of accidents involving breakdowns in sterile cockpit and
other procedures, including this accident and (2) obtain the input of operators and air carrier and
general aviation pilot groups in the development and distribution of these guidance materials. As
a result of this new recommendation, and because the FAA has not taken any action in 3 years to
address Safety Recommendation A-07-8, the recommendation is reclassified “Closed—
Unacceptable Action/Superseded.”
2.4.3 Crew Resource Management
Colgan provided CRM training to its pilots during initial and recurrent ground school.
The training addressed topics such as command, leadership and leadership styles,
communication, and decision-making. The training also included information on the importance
of maintaining situational awareness, employing checklist discipline, and adhering to standard
operating procedures. A CRM training instructor stated that the course also addressed the
relationship between flight crewmembers and the need to indicate when pilots were not
observing sterile cockpit procedures. The Colgan POI stated that the company’s training was
consistent with the guidance discussed in AC 120-51E, “Crew Resource Management Training.”
231
Safety Recommendation A-74-85 asked the FAA to “initiate a movement among the pilots associations to
form new professional standards committees and to regenerate old ones. These committees should: a) monitor their
ranks for any unprofessional performance, b) alert those pilots who exhibit unprofessionalism to its dangers and try,
by example and constructive criticism of performance required, to instill in them the high standards of the pilot
group, c) strengthen the copilot’s sense of responsibility in adhering to prescribed procedures and safe practices, and
d) circulate the pertinent information contained in accident reports to pilots through professional publications so that
members can learn from the experience of others.” Safety Recommendation A-74-86 asked the FAA to “develop an
air carrier pilot program, similar to the general aviation accident prevention program (FAA Order 8000.8A), that
will emphasize the dangers of unprofessional performance in all phases of flight. The program could be presented in
seminar form, using audio/visual teaching aids, to call to the pilots’ attention all facets of the problem.” Both
recommendations were classified “Closed—Acceptable Action” on March 10, 1977.

NTSB Aircraft Accident Report
104
Colgan’s CRM training should have provided the captain with the communication,
coordination, and resource management skills that were important to his role as PIC.
232
However, the captain did not effectively use all of the resources available to him to ensure safety
of flight. CRM training should also have provided the first officer with the skills to challenge the
captain’s deviations from standard operating procedures. The first officer was characterized
during postaccident interviews as being assertive, which was consistent with the CRM training
that she received. On the basis of the first officer’s level of involvement in conversations with
the captain, and the apparent ease with which they were communicating, it is unlikely that the
first officer’s failure to challenge the captain was because of a lack of assertiveness. It is possible
that she did not challenge the captain because she did not consider his deviations from standard
operating procedures to be remarkable. The NTSB concludes that the flight crewmembers’
performance during the flight, including the captain’s deviations from standard operating
procedures and the first officer’s failure to challenge these deviations, was not consistent with
the CRM training that they had received or the concepts in the FAA’s CRM guidance.
In late 2008, Colgan began the process of revising its CRM training. Even though the
training was consistent with the FAA’s CRM guidance, the Colgan POI and the company’s
director of flight operations, vice president of safety and regulatory compliance, and director of
crewmember and dispatcher training wanted to expand the program. In developing the revised
training, Colgan obtained guidance from Pinnacle Airlines and Continental Airlines.
The expanded CRM training program now spans 2 days (compared with the previous
initial and recurrent training programs, which lasted 8 and 2 hours, respectively). The revised
CRM program includes techniques for threat and error detection, management, and mitigation
and additional discussion of decision-making, leading and following, positively communicating,
and setting expectations. In addition, to facilitate discussion, the course is taught by line pilots
instead of ground instructors or management. During the summer of 2009, Colgan began
providing the revised recurrent CRM training to pilots, dispatchers, flight attendants, and
managers at its bases at EWR and IAH.
2.5 Fatigue
Although both pilots had flown during the week before the accident, their schedules were
within flight and duty time requirements and were not excessive in terms of accumulated flight
time or duty periods worked. However, each pilot made an inappropriate decision to use the
crew room to obtain rest before the accident flight, as discussed further in section 2.5.2.
According to his wife, the captain would typically sleep from about 2200 to 0900 and
would normally receive between 8 and 10 hours of sleep. (The captain’s wife explained that he
would awake earlier than 0900 for family activities.) From February 3 to 5, 2009, the captain
was working and had a duty period that started about 0500 and ended between 1200 and 1800
each day. The significantly earlier awakening time required for the report times, as well as being
232
As indicated in section 2.4.1, the NTSB has recommended the implementation of specific leadership
training for upgrading captains.
NTSB Aircraft Accident Report
105
away from home, would have produced some chronic sleep loss. However, the captain would
likely have been able to make up for this sleep loss while he was off duty and at home from
February 6 to 9.
On February 9, 2009, the captain commuted from his home in the Tampa area to EWR,
arriving about 2005 for a 2-day trip to begin the next day. His last known activity on February 9
ended about 2247. The captain was reported to have stayed overnight in the crew room at EWR.
On February 10 and 11, 2009, the captain had a report time of 0530, and his last known
activities those days ended between 2130 and 2200. As with his schedule 1 week before, the
captain’s earlier awakening time required for the report times, and his rest away from home,
would have produced some chronic sleep loss.
On the day of the accident, the captain was scheduled to report to EWR at 1330. Because
his duty period on February 11, 2009, had ended about 1544, he had a 21-hour, 16-minute
scheduled rest period before his report time. However, at 0310 on February 12, the captain
logged into Colgan’s CrewTrac computer system. This activity would have meant that he had, at
a minimum, a 5-hour opportunity for sleep followed by another sleep opportunity of about 4
hours. (The captain had logged into the CrewTrac system again at 0726.) The captain’s actual
sleep during this period is unknown. However, his sleep would have been further interrupted and
would likely have been of poor quality because he was again staying in the crew room.
233
As a
result, the captain would not have had an opportunity to restore his sleep loss from the previous 2
days. Also, it would have been difficult for the captain to nap in the crew room during the day
based on observations of his activities before the flight (which included office work, watching
television, and talking on the telephone or with other company pilots).
234
According to her husband, the first officer would go to sleep between 2000 and 2200 PST
and would awake between 0700 and 1000 PST. On February 4, 2009, the first officer commuted
from SEA to EWR because of the 5-day trip that she would be starting later that day. The duty
periods during the trip started between 1140 and 1235 (except for the first and last days, which
started at 1800 and 0825, respectively) and ended between 2049 and 0032 (except for the last
day, which ended at 1455).
235
The times of the trip (shown in eastern standard time) were mostly
consistent with the first officer’s PST home time zone.
236
However, it was possible that she had
accumulated some chronic sleep loss during this period because of the early awakenings required
for the report times on both the first day (as a result of her commute) and the last day of the trip,
as well as from being away from home.
233
This investigation found no evidence that the captain had stayed elsewhere that night.
234
According to Colgan’s Flight Operations Policies and Procedures Manual, the company’s dispatch release
requires each captain to confirm that he or she is “physically qualified for this flight.” The manual also stated that,
in signing this release, the captain was certifying that he or she is not fatigued and is physically capable of
completing the flight safely. The manual further indicated that, although other crewmembers, including first
officers, do not sign the dispatch release, it is a violation of company policy for any crewmember to conduct a flight
when fatigued or otherwise physically incapable of completing the flight safely.
235
The 0032 end time occurred in the middle of the trip and not before the 0825 start on the last day of the first
officer’s trip.
236
The first officer had moved from ORF (in the eastern time zone) to SEA 1 week before the trip but was
likely acclimated to the PST time zone.
NTSB Aircraft Accident Report
106
The first officer was home from February 9 to the morning of February 11. Her activities
each day began between about 0900 and 1000 PST and ended about 2230 PST, which would
have facilitated restoration of any sleep debt that she might have been experiencing. From about
1951 to about 2330 PST (0230 eastern standard time), the first officer traveled as a jumpseat
passenger on a cargo airplane from SEA to MEM and was reported to have slept 90 minutes
during the flight.
On February 12, 2009, from about 0418 to about 0623, the first officer traveled as a
jumpseat passenger on a cargo airplane from MEM to EWR and was reported to have slept the
entire flight. She was observed awake, and electronic records (telephone, text, and computer)
showed activity from the time of her arrival at EWR to about 0732. Afterward, no activities on
the part of the first officer were recorded until a text message she sent at 1305.
237
During the 24 hours that preceded the accident, the first officer was reported to have slept
3.5 hours on flights and 5.5 hours in the crew room. Although the opportunity for sleep
approached the first officer’s normal needs, her actual amount of sleep obtained is not known.
However, even if the first officer did obtain her normal amount of sleep, its quality would have
been diminished because of the manner in which it was obtained (on airplanes and in the crew
room). It is not known whether she received additional sleep by napping later in the day.
238
At the time of the accident, the captain would have been awake for at least 15 hours if he
had awakened about 0700 and for a longer period if he had awakened earlier. The accident
occurred about the same time that the captain’s sleep opportunities during the previous days had
begun and the time at which he normally went to sleep. The first officer had been awake for
about 9 hours at the time of the accident, which was about 3 hours before her normal bedtime.
The captain had experienced chronic sleep loss, and both he and the first officer had experienced
interrupted and poor-quality sleep during the 24 hours before the accident.
2.5.1 Role of Fatigue in Flight Crew Performance
For fatigue to be considered a factor in the flight crew’s performance, deficiencies need
to be clearly discernable and consistent with the known effects of fatigue, and any evidence
supporting alternative explanations for such deficiencies needs to be considered. Scientific
research and accident investigations have demonstrated the negative effects of fatigue on human
performance,
239
including reduced alertness and degraded mental and physical performance. For
237
The content of this text message indicated that the first officer had awakened from 6 hours of sleep.
238
The first officer’s opportunities for sleep at that time were reduced because of the recorded telephone, text,
and computer activity throughout the afternoon (see section 1.5.2.1).
239
For the scientific research, see J.A. Caldwell, “Fatigue in the Aviation Environment: An Overview of the
Causes and Effects as Well as Recommended Countermeasures,” Aviation, Space, and Environmental Medicine,
vol. 68, pages 932-938, 1997; D.R. Haslam, “The Military Performance of Soldiers in Sustained Operations,”
Aviation, Space, and Environmental Medicine, vol. 55, pages 216-221, 1984; and G.P. Kruger, “Sustained Work,
Fatigue, Sleep Loss, and Performance: A Review of the Issues,” Work and Stress, vol. 3, pages 129-141, 1989. For
the accident investigations, see, for example, the NTSB’s 1994 safety study on flight crew-involved major accidents
(referenced in section 2.3.1) and its report on the Corporate Airlines flight 5966 accident (referenced in section
1.18.1.1).

NTSB Aircraft Accident Report
107
example, breakdowns in vigilance can occur, response time can slow and become inaccurate,
decision-making and risk assessment can degrade, and motivation can decrease. In addition, task
management and prioritization can be affected by fatigue, and some reports have indicated a
reduction in leadership behavior with increased fatigue.
The pilots’ failure to detect the impending onset of the stick shaker and their improper
response to the stick shaker could be consistent with the known effects of fatigue. Workload
management issues, as well as some minor errors that occurred during the flight (for example, a
delayed response to an altitude alert about 2213:21) could also be consistent with fatigue.
However, the research and accident data have shown that the errors made by the flight
crewmembers, including their failure to monitor airspeed in relation to the position of the low-
speed cue, adhere to standard operating and sterile cockpit procedures, and respond
appropriately to the stick shaker, have also been observed in other pilots who were not fatigued.
It is important to note that, throughout the flight, the pilots were conversational and
engaged. Neither pilot acted withdrawn or lethargic or made any statements about being tired or
receiving inadequate sleep.
240
Also, the pilots demonstrated good performance during the flight
by following sterile cockpit procedures during the takeoff and initial climb. Other examples of
good performance by the flight crew include (1) the first officer’s detection, during her review of
the airplane’s logbooks, that a previous flight crew had not completed the 24-hour ice protection
check (the captain had just completed the check); (2) the captain’s interruption of his own
conversation to point out crossing traffic; and (3) his continuation of the approach briefing after
it was interrupted 50 seconds earlier by an ATC call.
Company pilots had reported that both accident pilots were competent in their positions
and adept with procedures and checklists. Also, the first officer had been described as being
assertive and ahead of the airplane as a monitoring pilot. Thus, both pilots’ performance failures
were inconsistent with these reports of their past performance, and, as stated in section 2.5,
evidence suggests that both pilots were likely experiencing some degree of fatigue at the time of
the accident. However, the errors and decisions made by the pilots cannot be solely attributed to
fatigue because of other explanations for their performance. For example, the fundamental
monitoring error made by the flight crew (the failure to recognize cues indicating the impending
stick shaker onset) was also made 1 month after the accident by another Colgan flight crew.
Also, the captain’s errors during the flight could be consistent with his pattern of performance
failures during testing, which he had experienced throughout his flying career. In addition,
research indicates that errors occur routinely during flight regardless of whether fatigue is
present and that errors are typically caught and mitigated by existing systems without serious
consequences.
241
240
Two yawns were recorded on the CVR during a 2-hour period. One was attributed to the captain about
2149:18; the other was attributed to the first officer about 2207:14.
241
J.R. Klinect, J.A. Wilhelm, and R.L. Helmreich, “Threat and Error Management: Data From Line
Operations Safety Audits,” Proceedings of the Tenth International Symposium on Aviation Psychology, Columbus,
Ohio: The Ohio State University, pages 683-688, 1999. M.I. Nikolic and N.B. Sarter, “Flight Deck Disturbance
Management: A Simulator Study of Diagnosis and Recovery From Breakdowns in Pilot-Automation
Coordination,” Human Factors, vol. 49, pages 553-563, 2007.

NTSB Aircraft Accident Report
108
Because the effects of fatigue can exacerbate performance failures, its role in the pilots’
performance during the flight cannot be ruled out. The NTSB concludes that the pilots’
performance was likely impaired because of fatigue, but the extent of their impairment and the
degree to which it contributed to the performance deficiencies that occurred during the flight
cannot be conclusively determined.
2.5.2 Industry Fatigue Mitigation Efforts
The NTSB has had a long-standing concern about the need to mitigate the effects of
fatigue in aviation. Reducing accidents and incidents caused by human fatigue has been on the
NTSB’s Most Wanted List since 1990. Also, the NTSB has issued numerous safety
recommendations addressing fatigue, including Safety Recommendation A-06-10, which was
issued on February 7, 2006, as part of the investigation of the Corporate Airlines flight 5966
accident. Safety Recommendation A-06-10 asked the FAA to do the following:
Modify and simplify the flight crew hours-of-service regulations to take into
consideration factors such as length of duty day, starting time, workload, and
other factors shown by recent research, scientific evidence, and current industry
experience to affect crew alertness.
On September 9, 2009, the FAA stated that an aviation rulemaking committee had
developed recommendations on flight and duty time limitations and rest requirements for
Part 121 and 135 operators. The FAA indicated that it was reviewing the recommendations
(which have not been publicly released) and that it had planned to publish a science-based
fatigue NPRM in December 2009.
242
On December 10, 2009, in testimony before the Subcommittee on Aviation, U.S. Senate
Committee on Commerce, Science, and Transportation, the FAA Administrator stated that the
FAA was reviewing the aviation rulemaking committee’s recommendations on flight and duty
time limitations and rest requirements but that additional analysis needed to be completed,
precluding the NPRM from being issued by the end of December 2009. The administrator also
stated that the NRPM would be published as soon as possible.
On December 29, 2009, the NTSB stated that the FAA, after years of inaction, appeared
to be on the verge of taking the recommended actions with regard to flight time limitations, duty
period limits, and rest requirements for Part 121 and 135 pilots. The NTSB noted that the FAA
had proposed publishing the NPRM in early 2010 but stated that the FAA had not informed the
NTSB of the specific revisions that the NPRM would include. Because the NTSB was not able to
determine at that time whether the revisions would fully satisfy the intent of Safety
242
The FAA’s last fatigue-based NPRM was 95-18, “Flight Crewmember Duty Period Limitations, Flight
Time Limitations, and Rest Requirements,” which was issued on December 20, 1995. The NTSB provided
comments on the NPRM, indicating that the proposed rule did not (1) include effective mechanisms to address flight
operations during the circadian night and circadian trough and (2) recognize the fatigue associated with multiple
takeoffs and landings. No changes in the rules regarding flight time and rest requirements were made after the
issuance of the NPRM. On November 23, 2009, the FAA officially withdrew the NPRM.
NTSB Aircraft Accident Report
109
Recommendation A-06-10, the recommendation remained classified “Open—Unacceptable
Response.”
One of the stated purposes of SAFO 06004 (previously discussed in sections 1.18.1.1 and
2.4.2) was to “call attention to fatigue as one of the most important elements to be addressed in
CRM training.” Even though the SAFO recommended that Part 121 directors of safety become
familiar with the document’s contents, a review of Colgan’s CRM course material at the time of
the accident showed only a minimal mention of fatigue. The company’s director of crewmember
and dispatcher training stated that fatigue was discussed as part of a review of situational
awareness. Also, Colgan personnel were not able to describe how the company had incorporated
the fatigue-related information in the SAFO.
Colgan had a nonpunitive fatigue policy in effect at the time of the accident
243
but did not
have a formal fatigue management program in place at the time. (Such a program was still not in
place as of January 2010.) After the accident, the company revised its CRM course material to
include a specific discussion of fatigue management and the hazards associated with fatigue.
Also, in April 2009, Colgan issued an operations bulletin to its pilots addressing the company’s
fatigue policy, causes of fatigue, recognition of fatigue and its effects on performance, and
prevention of fatigue by effectively using rest.
244
In December 2009, Colgan issued a read-and-sign memo to its pilots and flight
attendants, which stated that the company’s nonpunitive fatigue policy was being increasingly
abused. (As stated in section 1.17.5, the company indicated that crewmembers had been calling
in fatigued without a valid reason.) The memo also detailed interim changes to Colgan’s fatigue
policy. The memo stated that, effective December 31, 2009, fatigue calls would not be accepted
if a crewmember was returning from rest periods or personal time off duty (and did not properly
use the time off). The memo indicated that the safety department would consider mitigating
circumstances preventing a rest period from being fully utilized when evaluating a fatigue
call. In addition, the memo stated that the company was working with its pilot and flight
attendant unions to establish a comprehensive fatigue program, including a review board
process, by February 15, 2010.
At the public hearing for this accident, the FAA manager of air carrier operations stated
that fatigue mitigation in aviation was a joint responsibility between the operator and the pilot.
He also stated that company fatigue information can help pilots better manage their time off from
work. The accident pilots did not wisely manage their time off from work, which contributed to
the development of fatigue. In particular, the pilots chose to use the crew room during their rest
243
The policy allowed pilots to remove themselves from flight status without reprisals if they were too tired to
fly. Pilots calling in fatigued would not be paid for that flight segment if it were over their 75-hour monthly
guarantee. The company’s chief pilot indicated that the company tracked fatigue calls to identify trends but that no
consistent factors had been identified. Also, the Colgan POI had not received any complaints about the company’s
administration of the fatigue policy.
244
This information has also been incorporated into the Flight Operations Policies and Procedures Manual
revision, dated September 20, 2009. In addition, the NTSB notes that ALPA has developed resources for pilots on
preventing fatigue, recognizing fatigue symptoms, and mitigating the effects of fatigue.

NTSB Aircraft Accident Report
110
period, and their quality of sleep was affected by this decision.
245
Although the crew room was
supposed to be a quiet area with couches and recliners, it was not isolated and was subject to
interruptions, sporadic noise and activity, lights, and other factors that prevent quality rest. As a
result, neither pilot made use of the opportunity to obtain quality sleep and be as rested as
possible before the flight.
Company personnel stated that sleeping overnight in the crew room was against policy
because the room was not an adequate rest facility.
246
However, the captain used the crew room
for overnight sleeping on February 9 and 11, which indicates that the company was not
effectively enforcing its policy.
In addition, the first officer’s decision to begin a transcontinental commute about 15
hours before her scheduled report time without having an adequate rest facility affected her
ability to begin the trip as rested as possible. The commute from SEA to MEM and then from
MEM to EWR did not afford her an opportunity for an uninterrupted sleep period. Even though
the first officer arrived at EWR about 7 hours before her scheduled report time, this time period
was less than her normal sleep period, and evidence indicates that she could not have used all of
that time for sleep. Company guidance at the time of the accident, however, did not discourage
pilots from commuting on the same day that a trip was scheduled to begin.
247
The company’s commuting policy addressed ways to ensure that pilots were able to
arrive at their base and report for duty on time (see section 1.17.4), but the policy did not
reference ways to mitigate fatigue resulting from commuting. Testimony at the public hearing by
ALPA’s air safety chairman indicated that Colgan’s commuting policy was consistent with
industry practices.
Commuting is considered a privilege for air carrier pilots because they are not required to
live within a certain distance of their assigned base. Commuting may also be considered a
necessity for air carrier pilots because of possible changes in the industry, including base
closures, and the cost of living at some bases.
248
To accommodate the need for rest areas when
commuting, pilots often have “crash pads” (shared rooms or apartments) at their base if their
operator does not provide crew rest facilities for uninterrupted sleep. However, Colgan did not
have such a facility at EWR (or its other bases), and neither the captain nor the first officer had a
crash pad.
249
245
The NTSB notes that strategic napping in crew rooms during breaks is an effective countermeasure for pilot
fatigue and that this type of rest would be appropriate use of a crew room. However, the accident captain used the
EWR crew room for all of his sleep opportunity before the flight, and the first officer used the crew room for most
of her sleep opportunity.
246
The EWR regional chief pilot issued policy guidance in May 2008 stating that crewmembers were
responsible for their own overnight accommodations and that sleeping in the crew room was prohibited and would
have disciplinary consequences.
247
The previous edition of the Colgan Flight Crewmember Policy Handbook (dated February 2006) stated that
pilots should not commute to their base on the same day that they are scheduled to work. The handbook version
current at the time of the accident was dated March 2008 and did not include this guidance.
248
Colgan did not have locality pay for its pilots, but its management personnel received locality pay. In 2008,
the average salary of a company Q400 captain and first officer was $67,000 and $24,000, respectively.
249
Colgan does not require such an arrangement for its commuting pilots.

NTSB Aircraft Accident Report
111
Pilots who commute have a significant responsibility to make sure that they arrive fit for
duty and are able to maintain this fitness throughout the duration of their assigned duty period.
250
However, pilots who do not commute also have a responsibility to be fit for duty, and certain
circumstances can affect a noncommuting pilot’s ability to obtain adequate rest. For example, in
its investigation of the Federal Express flight 1478 accident in Tallahassee, Florida, the NTSB
found that the captain (who lived close to MEM, the departure airport) had received interrupted
sleep
251
during the two nights that preceded the accident because he had been taking care of the
family dog, whose health was deteriorating. The captain described his sleep during that time as
“marginal” and “not really good.” The captain reported that he had received 3.5 hours of “pretty
good” sleep before reporting about 0200 for the accident flight. The NTSB concluded that the
captain was likely impaired by fatigue and that the impairment contributed to his degraded
performance, especially in the areas of crew coordination and monitoring, during the approach to
the airport.
252
The NTSB notes that most pilots are cognizant of their personal responsibility to report to
work fit for duty, including having received the proper amount of rest. However, the
performance failures that occurred in the Tallahassee accident and this accident demonstrate the
negative outcomes that can occur when a pilot fails to obtain adequate rest before a flight. The
NTSB concludes that all pilots, including those who commute to their home base of operations,
have a personal responsibility to wisely manage their off-duty time and effectively use available
rest periods so that they can arrive for work fit for duty; the accident pilots did not do so by using
an inappropriate facility during their last rest period before the accident flight.
Companies can take actions to help mitigate fatigue in commuting pilots. Such actions
include providing rest facilities, providing assistance to pilots in identifying affordable
accommodations, planning flight schedules that support commuting without extended times of
wakefulness, and considering ways to evaluate and account for the effect of commuting on
subsequent duty periods. With regard to providing rest facilities, the FAA’s SAFO 09014,
“Concepts for Fatigue Countermeasures in Part 121 and 135 Short-Haul Operations,” issued on
September 11, 2009, stated that operators “should consider providing crew rest facilities that
have rooms away from the general traffic for quiet, comfortable and uninterrupted sleep.”
253
Most of Colgan’s EWR-based pilots (93 of 137 pilots) identified themselves as
commuters. However, the EWR regional chief pilot stated that he did not know the number of
commuting pilots at EWR. This lack of awareness is inconsistent with available information
stressing the importance of mitigating hazards associated with crewmember fatigue, including
SAFOs 06004 and 09014. The NTSB notes that, although many of the major accidents it has
250
Air transportation is one mode of transportation that pilots use to commute to their home base. Commuting
pilots can also use surface transportation to arrive at their base.
251
That captain had been released from duty on July 23, 2002, at 2353 and learned of the flight 1478
assignment on July 25 between 1800 and 1830.
252
For more information, see Collision With Trees on Final Approach, Federal Express Flight 1478, Boeing
727-232, N497FE, Tallahassee, Florida, July 26, 2002, Aircraft Accident Report NTSB/AAR-04/02 (Washington,
DC: NTSB, 2004).
253
SAFO 09014 also stated that pilots “should understand their responsibility with regard to ensuring that they
achieve the required rest so they are properly rested and fit for each assigned or scheduled flight.”

NTSB Aircraft Accident Report
investigated during the last decade involved pilots who commuted, this accident is the first one
in which the pilots’ rest location has been an issue. Operators have a fundamental responsibility
to support their pilots’ efforts to mitigate fatigue. However, Colgan did not (1) enforce the policy
prohibiting sleeping overnight in the crew room, which was an inappropriate rest facility for
uninterrupted sleep, and (2) have in place a formal fatigue management program. The NTSB
concludes that Colgan Air did not proactively address the pilot fatigue hazards associated with
operations at a predominantly commuter base.
On June 12, 2008, the NTSB issued Safety Recommendations A-08-44 and -45, which
asked the FAA to do the following:
Develop guidance, based on empirical and scientific evidence, for operators to
establish fatigue management systems, including information about the content
and implementation of these systems. (A-08-44)
Develop and use a methodology that will continually assess the effectiveness of
fatigue management systems implemented by operators, including their ability to
improve sleep and alertness, mitigate performance errors, and prevent incidents
and accidents. (A-08-45)
On August 11, 2008, the FAA noted that, in June 2008, it had hosted an international
symposium on fatigue in aviation operations to gather and make public the best available
knowledge on fatigue and fatigue mitigations. The FAA also stated that it was developing
operations specification guidance for fatigue management for ultra-long-range flights and that
lessons learned could likely benefit other flight profiles. On February 3, 2009, the NTSB
encouraged the FAA to ensure that guidance on fatigue management systems be developed for
all components of the aviation industry and not only for ultra-long-range operations. Safety
Recommendations A-08-44 and -45 were classified “Open—Acceptable Response” pending
such guidance.
A fatigue management system, also known as an FRMS, incorporates various
components and strategies to mitigate the hazards of fatigue in aviation operations. Components
of an FRMS include scheduling policies and practices, attendance policies, education, medical
screening and treatment, personal responsibility during nonwork periods, task and workload
issues, rest environments, commuting policies, and napping policies. An organizational plan for
implementing an FRMS and measuring its ability to mitigate fatigue is important to the success
of the system.
Many operators are beginning to implement components of an FRMS, and
countermeasures to address issues associated with commuting are expected to be part of an
FRMS. However, some operators have not adopted an FRMS, and neither FAA guidance nor
rulemaking currently exists in this area. As a result, the NTSB concludes that operators have a
responsibility to identify risks associated with commuting, implement strategies to mitigate these
risks, and ensure that their commuting pilots are fit for duty. Therefore, the NTSB recommends
that the FAA require all Part 121, 135, and 91K operators to address fatigue risks associated with
commuting, including identifying pilots who commute, establishing policy and guidance to
mitigate fatigue risks for commuting pilots, using scheduling practices to minimize opportunities
112

NTSB Aircraft Accident Report
113
for fatigue in commuting pilots, and developing or identifying rest facilities for commuting
pilots.
2.6 First Officer’s Illness Symptoms
According to the first officer’s husband and mother, the first officer was not sick when
she left home for her commute to EWR. In addition, pilots who spoke with and observed the first
officer during her commute and on the ground at EWR reported that she was not showing any
symptoms that were consistent with being sick. However, some of the accident pilots’ remarks
suggest that the first officer was experiencing symptoms associated with congestion or the onset
of a head cold. Also, the CVR recorded the first officer sniffling and sneezing multiple times
during the flight.
254
During the ground delay, the first officer stated, “I’m ready to be in the hotel room,” to
which the captain replied, “I feel bad for you.” The first officer continued, “this is one of those
times that if I felt like this when I was at home there’s no way I would have come all the way out
here.” She also stated, “if I call in sick now I’ve got to put myself in a hotel until I feel better …
we’ll see how … it feels flying. If the pressure’s just too much … I could always call in
tomorrow at least I’m in a hotel on the company’s buck but we’ll see. I’m pretty tough.”
During the descent, the pilots made some additional remarks regarding the first officer’s
symptoms. For example, the first officer stated, “might be easier on my ears if we start going
down sooner” Afterward, the captain asked the first officer about her ears, and she replied that
they were stuffy and popping.
Captains are responsible, as part of their initial crew briefing, for assessing the fitness for
duty of other crewmembers and for removing crewmembers from flight status if necessary. The
captain did not remove the first officer from flight status or question her remarks, so it is possible
that he did not think that her symptoms would affect her performance during the flight.
255
Postaccident toxicology testing on the first officer did not identify the presence of any
prescription or over-the-counter medications.
The NTSB attempted to determine whether the first officer’s symptoms would have
affected her performance during the flight. The sneezing, sniffles, and ear congestion could have
directly affected the first officer’s performance by interfering with communication. However, the
mistakes made during the accident sequence cannot be attributed to her symptoms. It is also
difficult to determine the extent of the first officer’s symptoms or their indirect effect on her
performance. In addition, the NTSB was not able to determine whether the first officer’s
symptoms contributed to her fatigued condition. Even with her comments about how she was
feeling, the first officer did state that she was “pretty tough,” and she was conversational and
254
The first officer’s husband stated that she would get sniffles from the cold air but that these sniffles were
not symptoms of a cold.
255
The CVR recorded the captain stating that the first officer could try an over-the-counter herbal supplement,
drink orange juice, or take vitamin C.
NTSB Aircraft Accident Report
114
engaged throughout the flight. As a result, the NTSB concludes that the first officer’s illness
symptoms did not likely affect her performance directly during the flight.
The NTSB, however, is concerned about the first officer’s reluctance to use Colgan’s
sick policy before the start of the trip. Company pilots were allowed to remove themselves from
flight status, without penalty, if they were sick.
256
If the illness began before the beginning of a
duty period, then the pilots would be responsible for their own accommodations. (In the first
officer’s case, she would have needed to pay for a hotel room until she felt well enough to return
to duty.) This situation illustrates the need for all commuting pilots to have adequate
accommodations, such as shared rooms or apartments, for obtaining rest (or recovering from the
onset of an illness) while at their home base and for operators to develop or identify rest facilities
for commuting pilots, as stated in Safety Recommendation A-10-16.
2.7 Captain’s Disapprovals and Training Problems
The captain had received several disapprovals and had experienced training problems
throughout his flying career.
257
In October 1991, the captain was disapproved for his initial
instrument airplane rating. The tasks disapproved were partial panel VOR approach, NDB
approach, and holding. During training for the instrument rating, a pilot is introduced to the
concept of attitude instrument flying (that is, the control of an aircraft’s spatial position using
instruments inside the cockpit rather than visual references outside the airplane). Instrument
training also teaches pilots to use a method known as cross-checking to continuously assess and
interpret the performance, control, and navigation of aircraft instruments. This training
establishes the foundation, skills, and habits a pilot uses for instrument flying.
All pilots must pass a checkride before a certificate or rating can be issued. Checkride
failures are not uncommon and are not necessarily an indication of incompetence.
258
Because the
captain’s initial instrument rating disapproval happened more than 17 years before the accident,
when he had only 125 hours total flight time, this failure was not especially significant. He
successfully completed the checkride 3.5 weeks later.
256
Colgan’s sick leave policy, which was adopted in June 2008, requested that pilots notify crew scheduling of
a sick call 2 hours before a flight. The vice president of administration stated that, if that were not possible, pilots
should not fly but cautioned that repeated events could be counted as a missed trip. Also, if pilots had not
accumulated sick time, then they would lose pay for the flight if it would put them over the 75-hour monthly
guarantee. (Section 1.17.5 discusses the sick leave earned by company pilots.) In addition, some commuting pilots
had been using sick leave when they were bumped from a flight and could not get to work. No evidence indicated
that this factor entered into the first officer’s decision-making, especially because the company had increased the
number of times that a pilot could receive relief from disciplinary actions under the commuting policy.
257
Even though the first officer was disapproved for her initial flight instructor certificate, the areas that
needed to be reexamined pertained to her instructional methods and abilities and not her flying skills. She passed the
test and was issued her certificate 5 days later.
258
FAA statistics for 2008 showed that 10.3 percent of all tested applicants for an additional rating were
disapproved, 28.5 percent of all tested applicants for an original commercial certificate were disapproved, and 9.4
percent of all tested applicants for an additional rating on a commercial certificate were disapproved. The 2008
overall failure rate for an original-issue FAA airline transport pilot certificate was 13.1 percent.

NTSB Aircraft Accident Report
115
In May 2002, the captain was disapproved for his initial commercial single-engine land
certificate.
259
The tasks disapproved were takeoffs, landings, go-arounds, and performance
maneuvers. The performance maneuvers required skillful control of altitude, heading, bank
angle, and airspeed. Failure to pass these tasks on a checkride could indicate poor control of the
airplane. After additional training, the captain passed the checkride 5 weeks later. At that time,
the captain had accumulated 296 hours total flight time.
In March 2004, the captain was disapproved for his initial commercial multiengine land
airplane certificate. The entire checkride needed to be repeated because the captain did not
perform enough maneuvers properly to get credit for them on a subsequent checkride. He
successfully completed the checkride on his next attempt 3 weeks later. The total number of
flight hours that the captain had accrued at that time was not recorded,
260
but his certificate
application for the rating showed that he had received 7.1 hours of flight instruction before the
test, which is minimal training for a multiengine certificate.
The captain’s disapproval for a commercial multiengine land airplane certificate was his
third successive failure to pass an initial attempt for an FAA certificate or rating, and it appeared
that his performance was not improving as he gained experience. In its September 9, 2005,
response to Safety Recommendation A-05-2 (see section 1.18.1.8), the FAA stated that multiple
checkride failures showed no correlation with pilots’ accident and incident records. However, the
captain’s established pattern of first-attempt failures might have indicated that he was slow to
absorb information, develop skills, and gain mastery or that the training he received was not
adequate. This pattern might also have indicated that the captain had difficulty performing
required skills while under the stress conditions associated with a checkride.
The captain attended Gulfstream Training Academy from August 2004 to April 2005 and
completed initial training at GIA (which was directly associated with the academy) in December
2004. Details from his training records, however, revealed his continuing difficulties with
aircraft control. During two simulator periods, he was graded unsatisfactory in “approach to stall
– landing configuration.” During a later simulator period, he demonstrated unacceptable altitude
and airspeed control. During the final planned simulator session, the instructor noted basic
attitude flying problems and repeated deviations. Because additional training was required, an
extra simulator session occurred the next day. All maneuvers were graded satisfactory at that
time. The simulator checkride occurred the same day as the additional training.
The captain’s GIA training records clearly showed that his flying skills needed
improvement, but he had apparently met the minimum standards required for completion of the
training. Thus, he began flying the BE-1900D as a fully qualified first officer. However, the
captain’s GIA training records should have raised concerns about his suitability for employment
at a Part 121 air carrier.
259
Standards of execution are higher for a commercial pilot certificate than for a private pilot certificate.
260
FAA medical records showed the captain reported 300 hours total flight time (with no hours during the
previous 6 months) on his medical certificate application dated January 16, 2004. He reported 325 flight hours (with
25 hours accrued during the previous 6 months) on his medical certificate application dated July 27, 2004.

NTSB Aircraft Accident Report
116
The captain applied to Colgan in August 2005 and was hired the next month. At that
time, the captain had 618 total flight hours, 290 of which were accumulated while at GIA in a
multiengine airplane. His total number of flight hours met the company’s internal policy
requirements at the time, which were a minimum of 600 hours total time, including 100 hours of
multiengine time.
261
This minimum was typical for new hires at regional airlines at that time.
The Colgan employment application asked the question, “have you ever failed any
proficiency check, FAA check ride, IOE or line check?” The captain responded, “yes, FAA
check ride for instrument rating. I missed the NDB approach, received additional instruction,
then repeated the approach and passed.” He did not disclose the two other certificate
disapprovals that he had received. At the public hearing for this accident, the company’s vice
president of administration stated that, if the captain’s incomplete answer had previously been
known, it would have resulted in his dismissal from the company.
262
The captain’s initial proficiency check at Colgan, as a first officer on the Saab 340,
occurred in October 2005. The captain was graded “train to proficiency” for normal and
abnormal procedures. This grade indicated that the captain had completed the checkride but
needed additional training on normal and abnormal procedures before he would be considered
fully successful. Colgan could not provide any further details about this event.
In October 2006, the captain received an unsatisfactory grade on his next flight check,
which was his first recurrent proficiency check as a first officer in the Saab 340. The
unsatisfactory tasks were rejected takeoffs, general judgment, landings from a circling approach,
oral exam, and nonprecision approach. According to company records, the captain attended
recurrent training and then completed requalification proficiency training the next month.
However, no evidence showed that Colgan considered the captain’s performance (as a Saab 340
first officer) to be a concern, even with the problems he demonstrated during the initial and
recurrent proficiency checks.
The captain began upgrade training on the Saab 340 in October 2007 and attempted a
checkride for an FAA airline transport pilot certificate and type rating later in the month, but he
was initially disapproved. The check airman indicated that the captain’s airspeed was too slow
on a second missed approach while attempting to complete a single-engine ILS approach. After
another check airman provided further training for the captain, the original check airman
conducted the recheck and approved the captain for the certificate and type rating 3 days later.
Even though the captain had demonstrated problems with the three checkrides he had
performed, Colgan was not proactively addressing his training and proficiency issues. For
example, the company’s director of flight standards stated that he had not tracked the captain in
terms of his performance. Also, the company’s chief pilot stated that he could not recall talking
to anyone at the company about the captain’s training record. The chief pilot further stated that
261
On April 30, 2009, Colgan began requiring newly hired pilots to have a minimum of 1,000 hours total flight
time and 100 hours in multiengine aircraft.
262
The company stated that its current employment policy does not consider pilots with more than one failed
checkride.

NTSB Aircraft Accident Report
117
he was aware of the captain’s initial upgrade failure in the Saab 340 and that he told the captain
that his next proficiency check needed to be “right on.”
The captain had satisfactorily completed recurrent proficiency training in April 2008 and
a line check in September 2008, indicating that his mastery of the Saab 340 was improving. The
chief pilot approved the captain for Q400 transition training,
263
which he began in October 2008.
The captain had satisfactorily completed his line-oriented flight training, IOE, line check, and
type rating.
264
However, at the time of the accident, the captain had been flying the Q400 for just
over 2 months and thus was still new to the airplane.
Interviews with Colgan instructors revealed that, even though the captain had progressed
significantly in terms of his confidence, crew management, and execution of procedures, some of
his problems with aircraft control remained. For example, the Q400 simulator instructor stated
that, during unusual attitude training, the captain was “very rough” on the controls and had
somewhat overcontrolled the roll axis.
The basic concept of attitude instrument flying involves making the proper adjustments
to flight and power controls to control aircraft attitude. The NTSB concludes that the captain had
not established a good foundation of attitude instrument flying skills early in his career and that
his continued weaknesses in basic aircraft control and instrument flying were not identified and
adequately addressed.
2.7.1 Remedial Training and Additional Oversight
Because of his continued weaknesses in basic aircraft control and attitude instrument
flying, the captain would have been a candidate for remedial training. However, at the time of
the accident, the company did not have a formal program for pilots who demonstrated ongoing
weaknesses. The company’s director of flight standards stated that pilots who were found to be
unsatisfactory because of a failed checkride could retrain on the specific failure item and that no
further followup would occur if the pilot were found to be satisfactory on the subsequent
checkride. This director also stated that, for pilots with multiple unsatisfactory checkrides, he or
the flight standards manager would coordinate with the director of crewmember and dispatcher
training to assign additional training. (As stated in section 1.17.1.3, Colgan began a formal pilot
monitoring program in August 2009.)
Even though the captain had failed two checkrides since beginning work for Colgan (and
was graded “train to proficiency” on another checkride), he had received retraining on the
specific failure items and then subsequently passed the checkrides. As a result, no additional
training or overall review of his skills as a pilot occurred.
263
The chief pilot stated that the captain’s record did not show anything significant that would have prevented
him from successfully transitioning to the Q400.
264
The check airman who conducted the captain’s initial proficiency check on the Q400 indicated that he did
well on the oral portion of the check and was “well above average” in the simulator. The check airman further stated
that the captain completed his transition IOE without difficulty, except that he was somewhat slow in adapting to
the flight management system.

NTSB Aircraft Accident Report
During its investigation of the Federal Express flight 647 accident, the NTSB found that
the company had an oversight program that identified flight crewmembers with demonstrated
performance deficiencies or training failures and provided them with additional oversight and
training. The NTSB’s report on the accident (see section 1.18.1.7) concluded that such a
proactive program would benefit flight safety at other Part 121 carriers. As a result, on May 31,
2005, the NTSB issued Safety Recommendation A-05-14, which asked the FAA to do the
following:
Require all 14 Code of Federal Regulations Part 121 air carrier operators to
establish programs for flight crewmembers who have demonstrated performance
deficiencies or experienced failures in the training environment that would require
a review of their whole performance history at the company and administer
additional oversight and training to ensure that performance deficiencies are
addressed and corrected.
On April 13, 2007, the FAA stated that it had issued SAFO 06015, “Remedial Training
for Part 121 Pilots,” on October 27, 2006. The purpose of the SAFO was to promote voluntary
implementation of remedial training for pilots with persistent performance deficiencies. The
SAFO recognized that many air carriers had voluntarily incorporated remedial training to
supplement their approved training programs and that these remedial training programs were
effective in addressing and correcting below-standard pilot performance. For air carriers without
a voluntary remedial training program, the SAFO recommended implementing a process to
identify pilots with persistent performance deficiencies and/or multiple failures during training
and checking. The SAFO advised that this process should (1) review the entire performance
history of any pilot in question, (2) provide additional remedial training as necessary, and (3)
provide additional oversight by the air carrier to ensure that performance deficiencies were
effectively addressed and corrected.
On December 12, 2007, the NTSB stated that the FAA needed to survey all Part 121
operators to determine whether they had taken the action recommended in SAFO 06015. Safety
Recommendation A-05-14 was classified “Open—Acceptable Alternate Response” pending
completion of this survey and demonstration that all Part 121 carriers had programs to address
pilot performance deficiencies or failures during training.
On April 23, 2009, the FAA issued Notice 8900.71, which discussed verification of
remedial training for Part 121 carriers. The purpose of the notice was to provide guidance to
POIs about a required inspection to determine whether their Part 121 carriers were voluntarily
complying with SAFO 06015. The notice also instructed the POIs to complete the inspection
within 90 days of the date of the notice. During the public hearing for this accident, the POI for
Colgan stated that he was not aware of SAFO 06015.
By definition, SAFOs are advisory only, and the decision to implement a SAFO rests
with an operator. The NTSB notes that SAFO guidance may be an acceptable alternate response
to a safety recommendation if an FAA survey finds that all of the operators have implemented
the recommended actions. However, during public hearing testimony, the FAA’s manager of air
carrier training indicated that he did not know which carriers had complied with SAFO 06015.
118

NTSB Aircraft Accident Report
119
On October 30, 2009, the FAA indicated that 29 of the 82 Part 121 carriers and 2 of the
24 Part 121/135 carriers had implemented the actions recommended in SAFO 06015. The total
number of Part 121 carriers included 27 regional carriers, 6 of which had implemented the
SAFO’s recommended actions. On December 10, 2009, the FAA Administrator stated, during
his testimony before the U.S. Senate, that two-thirds of the air carriers without advanced
qualification programs
265
had systems in place to identify and manage low-time pilots and pilots
with persistent performance problems. The administrator also stated that, for those carriers
without such systems, additional FAA oversight of their training and qualification programs
would be conducted. The FAA’s January 27, 2010, fact sheet regarding its “Call to Action”
report stated that all air carriers (including the 14 carriers that had advanced qualification
programs) had developed remedial training programs for pilots that were consistent with the
guidance in SAFO 06015.
The NTSB concludes that remedial training and additional oversight for pilots with
training deficiencies and failures would help ensure that the pilots have mastered the necessary
skills for safe flight. Because the NTSB has not determined the extent that air carrier remedial
training programs address pilot performance deficiencies and failures during training, the NTSB
reiterates Safety Recommendation A-05-14.
2.7.2 Pilot Training Records
During the investigation of this accident, the NTSB found discrepancies between the
dates entered into Colgan’s electronic training record system and those in the FAA’s certificate
records. Specifically, the company’s records showed that the captain had failed his initial
upgrade proficiency check on the Saab 340 on October 3, 2007, received upgrade line-oriented
flight training and upgrade simulator training on October 14, received additional simulator
training on October 15, and passed his upgrade proficiency check on that same day. However,
FAA certificate records showed that the captain failed his initial Saab 340 upgrade proficiency
check on October 15 and passed the check on October 18.
Because Colgan used an electronic record-keeping system to maintain training records
for pilots, detailed paper training records were destroyed once the information was entered into
the system.
266
As a result, the NTSB was not able to reconstruct the actual sequence of events
concerning the captain’s Saab 340 upgrade proficiency check. Colgan’s director of crewmember
and dispatcher training stated that the discrepancy between the company’s and the FAA’s dates
was the result of a clerical error. However, a discrepancy also existed within the company.
Specifically, the check airman who conducted the captain’s two upgrade proficiency checks
265
An advanced qualification program is a voluntary alternative to the traditional regulatory requirements
under Parts 121 and 135 for pilot training and checking.
266
The NTSB’s investigation of a May 2003 accident involving Colgan showed that the company was
retaining detailed paper records at that time. (The accident involved a Colgan Saab 340B, N277MJ, and a Dassault
DA-50, N664B, at LaGuardia Airport, Flushing, New York. The NTSB determined that the probable cause of the
accident was the inadequate visual lookout and inadequate crew coordination of the Dassault DA-50 flight crew
while taxiing, which resulted in a ground collision with the taxiing Saab 340B.) Additional information about this
accident, NTSB case number NYC03LA114A, is available on the NTSB’s website at
<http://www.ntsb.gov/ntsb/query.asp>.

NTSB Aircraft Accident Report
120
stated that the second check was conducted the day after he failed the first check, but the
company’s electronic records indicated that the second check was conducted 12 days after the
failure. These discrepancies in the captain’s training records were notable because he had
demonstrated previous training difficulties at the company and the events surrounding his
upgrade proficiency check warranted further scrutiny.
The company’s electronic training record system contained only a basic description of
each training event, along with codes for specific items, including the type of airplane, crew
position, and instructor name, and a brief statement of any maneuver that was performed
unsatisfactorily. If a company manager wanted to reconstruct events from a pilot’s training, the
manager would need to contact the instructor or check airman who conducted that training.
However, interviews with instructors and check airmen who had trained the accident flight crew
revealed that some of them could not remember specific details about training events, including
the check airman who graded the captain as train to proficiency on his 2005 initial Saab 340
proficiency check and as unsatisfactory on his 2006 recurrent Saab 340 proficiency training.
Thus, an air carrier cannot depend solely on the memory of instructors and check airman to
identify trends in a pilot’s performance.
Colgan’s Crewmember and Dispatcher Training Program Manual specified a grading
legend to indicate a pilot’s performance on each training maneuver.
267
The electronic training
record system did not include these grades, even though this information could help company
managers determine a pilot’s progress during training or events that needed repetitive training.
Instructor comments at the time of the training are another source of valuable information
regarding a pilot’s performance, but such comments were also not included in the company’s
electronic training record system.
During its investigation of the American Eagle flight 3379 accident, the NTSB was
unable to locate instructor comments about the quality of the captain’s performance during
activities that trained or assessed pilot skills and found that the air carrier’s management was
unaware of critical aspects of the captain’s performance. As a result, on November 15, 1995, the
NTSB issued Safety Recommendation A-95-116, which asked the FAA to require all air carriers
and their training facilities to maintain pertinent information on the quality of pilot performance.
On April 17, 1998, the FAA stated that the inclusion of subjective evaluations by individual
instructors, check airmen, or FAA inspectors in a pilot’s permanent record might make a training
event a punitive experience rather than one in which a pilot could learn from mistakes. On
January 3, 2000, the NTSB stated that the FAA had provided a convincing argument about the
inappropriateness of subjective information in pilot records and the possibility that pilot training
could be negatively affected and classified the recommendation “Closed—Reconsidered.”
Detailed paper records of the captain’s performance at his previous airline, GIA, were
obtained during the investigation. These records provided greater insight into the captain’s
267
Grading was done on a scale of one through four. Grades of one and two indicated that the pilot understood
the maneuver and completed it successfully; a grade of one was given when no further training was necessary, and a
grade of two was given if further training for retention was necessary. A grade of three indicated that the pilot
understood the maneuver but did not complete it satisfactorily and that further training was necessary. A grade of
four indicated that the pilot did not understand the maneuver or complete it satisfactorily and that further instruction
and explanation was needed before further flight or simulator training.

NTSB Aircraft Accident Report
performance than the records maintained by Colgan. For example, remarks in the captain’s
training record at GIA included “airspeed 10 knots below Vref,” “repeated deviation from
altitude 200-300 feet,” and “constant deviations up to full scale on glide slope.” It is important to
note that these remarks were not subjective evaluations (about which the FAA expressed concern
in its response to Safety Recommendation A-95-116); rather, these remarks were criteria-based
observations that provided an explanation for the captain’s unsatisfactory performance and his
need for further training in attitude instrument flying.
At the public hearing for this accident, the POI for Colgan stated that, although the
company’s training records met regulatory requirements, he was concerned about the lack of
detailed information in the system. The FAA’s manager of air carrier training stated that
electronic record-keeping systems, such as the one used by Colgan, were approved individually
for each air carrier by its POI and that his branch, which sets FAA policy on training, does not
approve “software of that nature as a standalone item.” The FAA manager also indicated that the
agency did not require training records to be verified or validated but stated that there should be
a way to audit and amend records before they appeared in their final format.
The NTSB notes that the use of electronic pilot training records is acceptable as long as
the records contain detailed information from which a pilot’s performance during training and
checking events can be fully determined. However, the NTSB concludes that Colgan Air’s
electronic pilot training records did not contain sufficient detail for the company or its POI to
properly analyze the captain’s trend of unsatisfactory performance. Therefore, the NTSB
recommends that the FAA require Part 121, 135, and 91K operators to document and retain
electronic and/or paper records of pilot training and checking events in sufficient detail so that
the carrier and its POI can fully assess a pilot’s entire training performance. The NTSB also
recommends that the FAA require Part 121, 135, and 91K operators to include the training
records requested in Safety Recommendation A-10-17 as part of the remedial training program
requested in Safety Recommendation A-05-14. The NTSB further recommends that the FAA
require Part 121, 135, and 91K operators to provide the training records requested in Safety
Recommendation A-10-17 to hiring employers to fulfill their requirement under PRIA. In
addition, the NTSB recommends that the FAA develop a process for verifying, validating,
auditing, and amending pilot training records at Part 121, 135, and 91K operators to guarantee
the accuracy and completeness of the records.
2.7.3 Pilot Records Improvement Act
Colgan’s vice president of administration stated that, as part of a pilot applicant’s
background check, the company checked the paperwork required by PRIA (see section 1.18.2.1)
but that many of the pilots hired by the company did not have previous experience with other
airlines, so the information required under PRIA would not be available for them. However, as
noted previously, the captain had failed, on three separate occasions, to pass an FAA checkride
on his initial attempt. On his application for employment with Colgan, the captain acknowledged
only one of the failures. PRIA requirements and FAA guidance (AC 120-68C, “Pilot Records
Improvement Act of 1996,” dated January 28, 2004) in place at the time that the captain was
121

NTSB Aircraft Accident Report
hired did not require operators to obtain notices of disapproval for flight checks for certificates
and ratings.
On January 27, 2005, the NTSB issued Safety Recommendation A-05-1 as a result of the
accident involving Air Sunshine flight 527 in Treasure Cay, Great Abaco Island, Bahamas.
Safety Recommendation A-05-1 asked the FAA to “require all Part 121 and 135 air carriers to
obtain any notices of disapproval for flight checks for certificates and ratings for all pilot
applicants and evaluate this information before making a hiring decision.”
On September 9, 2005, the FAA stated that requiring all Part 121 and 135 air carriers to
obtain these notices would necessitate FAA rulemaking or a change to the PRIA statute. Instead,
the FAA stated it would amend AC 120-68C to indicate that a letter of consent signed by a pilot
applicant could be used to authorize the FAA to release records of notices of disapproval for
flight checks for certificates and ratings to an air carrier making such a request. On November 3,
2006, the NTSB stated that, because the AC information was not mandatory, the FAA needed to
survey operators to determine how many were obtaining airman certification records for their
pilot applicants from the FAA so that the effectiveness of the FAA’s planned action could be
assessed. The NTSB classified this recommendation “Open—Acceptable Alternate Response”
pending results from the survey and the revision of AC 120-68C.
On November 7, 2007, the FAA issued AC 120-68D, which contained the following
information in bold print:
A request with a signed consent by the pilot/applicant may be used to authorize
the FAA to release records of Notices of Disapproval for flight checks for
certificates and ratings to an air carrier making such a request. Air carrier
representatives involved in the pre-employment screening process may find this
additional information helpful in evaluating the pilot/applicant. These requests,
however, are not an integral part of the standard PRIA request process.
At the public hearing for this accident, the FAA’s program manager for PRIA stated that
air carriers have always had the ability to request records from the FAA beyond those required
by PRIA as long as the carriers obtained a signed consent statement from the pilot applicant (as
highlighted by the revised AC on PRIA). The program manager stated that he did not know how
many air carriers had obtained additional FAA airman certification information for their pilot
applicants, but he stated that only one or two air carriers had contacted him for such information.
The FAA’s manager for air carrier certification also stated that he did not know how many
operators were obtaining these data because the survey that the NTSB requested in its
November 2006 letter has not been conducted.
The NTSB continues to believe that airman certification information concerning previous
notices of disapproval should be included in an air carrier’s assessment of the suitability of a
pilot applicant. The NTSB also considers notices of disapproval to be safety-related records that
must be included in an air carrier’s evaluation of a pilot’s career progression, along with the
detailed training records requested in Safety Recommendations A-10-17 through -20. The
revision to AC 120-68 is an interim solution for this safety issue; however, a more permanent
action through rulemaking would ensure that air carriers would be required to obtain and
122

NTSB Aircraft Accident Report
evaluate notices of disapprovals for pilot applicants. The NTSB concludes that notices of
disapproval need to be considered along with other available information about pilot applicants
so that air carriers can fully identify those pilots who have a history of unsatisfactory
performance. Because of the FAA’s failure to demonstrate voluntary compliance with the
advisory information in AC 120-68D, the NTSB reiterates Safety Recommendation A-05-1 and
reclassifies it “Open—Unacceptable Response.”
In addition, although AC 120-68D had not been issued when the captain was a pilot
applicant, Colgan could have still obtained a signed consent statement from him that would have
allowed the company to obtain and review his three notices of disapproval. As previously stated,
Colgan’s vice president of administration indicated that, if the company had known about the
captain’s complete history of FAA checkride failures, then he would have been dismissed from
the company. Also, Colgan did not obtain a signed consent statement from the first officer when
she was a pilot applicant, even though she was hired after AC 120-68D had been issued. As a
result, the NTSB concludes that Colgan Air did not use all available sources of information on
the flight crew’s qualifications and previous performance to determine the crew’s suitability for
work at the company.
2.8 Airspeed Selection Procedures
Bombardier specified procedures for the use of the ref speeds switch in the Q400 AFM,
which is an FAA-required document. The AFM’s procedures for use of the ref speeds switch
were included in a section about ice protection features. As discussed in sections 1.17.2.2 and
2.2.2, the procedures indicated that the ref speeds switch was to be turned to the increase
position before entering icing conditions or upon initial detection of icing and was to be turned
to the off position when the airplane was aerodynamically clean (that is, all ice was removed
from the visible leading edges of the wing and wing tips). For a flaps 15 landing with the ref
speeds switch in the increase position, pilots needed to increase airspeeds by 20 knots.
Q400 operators were responsible for developing their own procedures for the use of the
ref speeds switch that were consistent with the AFM and approved by the FAA. Colgan’s
procedures for the Q400 were summarized in its CFM, which provided the normal procedures
and checklists for flight crews. However, the only direct or indirect references in the Q400 CFM
regarding how and when to use the ref speeds switch were the following:
• In the expanded portion of the after start checklist, which is accomplished before
takeoff, a caution note stated, “Ensure the REF SPEEDS switch is set to OFF. If REF
SPEEDS switch is set to INCR, the stick shaker may activate on takeoff.”
• An item on the expanded portion of the climb checklist was “ice protection – as
req’d,” with the remark, “make sure de-icing and anti-icing switches are set as
required for the ambient conditions.”
• An item on the cruise checklist was “24-hr ice protection test – as req’d.” (As
previously indicated, the ref speeds switch was one of the items to be checked.)
123

NTSB Aircraft Accident Report
124
During postaccident interviews, Colgan pilots indicated that they were familiar with the
function and operation of the ref speeds switch. However, some company pilots expected to be
able to turn off the switch before the approach and landing flight phases, as the airplane
descended out of icing conditions. For example, one pilot stated that he had turned the ref speeds
switch to the off position after descending out of icing conditions but had planned to “mentally”
add 20 knots to the airspeed if ice had resumed on final approach. The captain of the BTV stick
shaker event stated that she had briefed the landing speeds based on the expectation that the ref
speeds switch would be turned to the off position before the beginning of the approach, but she
had forgotten to turn the switch to off, and the first officer had not noticed the position of the
switch.
Even though the ref speeds switch is relatively uncommon among air carrier airplanes,
268
it is still important for the switch to be properly matched to the airspeed bugs on those airplanes
with the switch installed. In the Q400, airspeed bugs are set by pilots using a rotary knob on their
outboard forward panel. Two bugs are available for landing, but the AFM does not require their
use or specify how they should be set.
The NTSB found that Q400 operators used different bug speeds for landing. One
operator, which had operated the airplane for 10 years, instructed its pilots to set the two
available bugs to V
ref
and V
ref
(ice)
for every approach to prevent confusion or the need to reset
bugs during an approach if conditions were to change. Another operator, whose director of flight
operations was previously a Q400 certification test pilot, had its pilots set the landing bugs to
V
ref
and V
ga
partly because landings accomplished with the higher (icing) reference speed were
rare. This operator found that, even when operating during wintertime in a northern climate,
most conditions at 1,000 feet agl were such that the landing could be conducted at normal
reference speeds.
Colgan chose to have its pilots set either V
ref
or V
ref
(ice)
and V
ga
as the landing bugs. If
V
ref
had been set and icing conditions were encountered, or if V
ref
(ice)
had been set and the
airplane was no longer in icing conditions, each pilot was expected to manually reset the
airspeeds.
Colgan’s guidance on setting landing bugs was contained in the CFM expanded approach
checklist. The guidance indicated that pilots were to determine the landing weight and airspeeds
and then set the solid blue bug to V
ref
or V
ref (ice)
and the open blue bug to V
ga
. Both flight
crewmembers were to verify this action by responding “set.” This procedure did not mention
cross-referencing the airspeed bug settings with the ref speeds switch position (which are
independent of each other) and did not include information about the early stall warning that
could result from setting normal V
ref
speeds with the ref speeds switch in the increase position.
After the accident, Colgan issued two operations bulletins pertaining to the ref speeds
switch and airspeed settings.
269
The first bulletin, 09-001, included two warnings and two
cautions under the heading, “ref speeds switch.” The warnings prohibited (1) moving the ref
268
The NTSB is not aware of any air carrier airplanes that have a ref speeds switch besides the Q400, which is
operated by two other U.S air carriers in addition to Colgan.
269
The first bulletin was issued before the BTV event, and the second one was issued after the event.

NTSB Aircraft Accident Report
125
speeds switch to the increase position below 1,000 feet agl during takeoff and (2) changing the
position of the ref speeds switch below 1,000 feet agl during landing. The cautions indicated that
(1) if airspeed is within 20 knots of the low-speed cue, then the airspeed must be increased
before the ref speeds switch is selected to the increase position, or a stall warning might occur,
and (2) if V
ref
is used for landing, then the ref speeds switch must be selected to the off position,
or a stall warning might occur at an airspeed higher than V
ref
. The bulletin also added a specific
response to any ice protection system checklist item and required both flight crewmembers to
respond, and it reiterated the proper icing terminology to use with the ACARS system (“icing” or
“eice”)
270
to ensure that the proper ice speeds were received (from AeroData) for V
ref
and V
ga
.
The second bulletin, 09-003, added a specific line item to the approach checklist, “ref
speeds switch – as req’d,” with both crewmembers responding. It also provided guidance to
flight crews, including a requirement to decide on the position of the switch before the initial
approach phase, a prohibition against changing the switch position below 1,000 feet agl, a
requirement to use only V
ref
(ice)
and V
ga
(ice)
with the ref speeds switch set to the increase
position, and a statement that the speed bugs could be reset to V
ref
and V
ga
if the ref speeds
switch was turned to the off position above 1,000 feet agl. A reference to the switch was added
to the takeoff profile, and the approach profiles were changed to require a minimum airspeed of
180 knots before lowering the landing gear.
Colgan’s flight crew training on the use of the ref speeds switch was incorporated into its
ground school curriculum. An examination of the company’s slides used during Q400 initial
training showed that the function of the ref speeds switch was described in the module on the ice
and rain protection system. However, the actual use of the ref speeds switch was not included in
the modules on AeroData, ACARS, line-oriented flight training, situational awareness and
safety, or winter operations.
271
Colgan’s training manual, which contained the syllabus for Q400 upgrade and transition
training, did not specifically mention the ref speeds switch in ground school subject matter
sections, including the one on ice and rain protection. Also, the simulator training modules
described in the manual made no direct reference to the use of the ref speeds switch. Thus, it is
unlikely that crews were appropriately trained on the use the ref speeds switch, especially during
simulator training, when it is important for pilots to demonstrate an understanding of the need to
match the approach speed bug settings to the position of the ref speed switch.
The NTSB acknowledges Colgan’s efforts after the accident to educate its flight crews,
through CFM operations bulletins, about the relationship between the ref speeds switch and
airspeed bug settings. However, training in this area would further emphasize this relationship.
The NTSB concludes that Colgan Air’s procedures and training at the time of the accident did
not specifically require flight crews to cross-check the approach speed bug settings in relation to
270
Before the accident, the CFM showed these terms, which could be used in the optional remarks field of the
landing condition screen, but the manual did not elaborate on the effect that the entries would have on the airspeed
and landing distances received. Also, the CFM did not mention the need to cross-reference the position of the ref
speeds switch when requesting landing performance data using either of the terms.
271
Colgan’s ground school training included slides on ACARS and winter operations. However, specific
information about entering icing terminology into ACARS and the relationship of these entries to the stall warning
and the ref speeds switch were not discussed.

NTSB Aircraft Accident Report
126
the ref speeds switch position; such awareness is important because a mismatch between the
bugs and the switch could lead to an early stall warning. Therefore, the NTSB recommends that
the FAA direct Part 121, 135, and 91K operators of airplanes equipped with a ref speeds switch
or similar device to (1) develop procedures to establish that, during approach and landing,
airspeed reference bugs are always matched to the position of the switch and (2) implement
specific training to ensure that pilots demonstrate proficiency in this area.
2.9 Stall Training
During training for private and commercial certificates, pilots perform recoveries from
fully developed stalls. Even though these stall recoveries are typically accomplished in small
trainer-type airplanes, the sensations and lessons from this training usually remain with a pilot.
However, as pilots transition to larger, autopilot-equipped, transport-category airplanes, they
rarely, if ever, receive reinforcement of how actual stalls feel and how they are to be handled
because air carrier training does not require pilots to practice recoveries from fully developed
stalls.
The airline transport pilot practical test standards provide explicit guidance regarding
how airline pilots should enter, induce, and recover from an impending stall (known as an
approach to stall) but not a full aerodynamic stall. The approach-to-stall maneuvers require strict
adherence to precise airspeed, altitude, and heading control and continuous smooth positive
control. Colgan’s training manual referenced the practical test standards in its procedures for
stall training, and training records indicated that the accident pilots had met these standards
during their Q400 training.
272
The practical test standards currently require pilots to recover from an approach to stall
with minimal altitude loss. This recovery procedure can be effective as long as an airplane is not
fully stalled. However, altitude loss standards are not an appropriate method for determining if a
pilot can recognize and properly respond to a fully developed stall. Once a stall has occurred, an
airplane cannot be recovered until the wing’s AOA is reduced, which will necessitate a loss of
altitude. At stall AOAs, drag is high, and the thrust available may not be sufficient to overcome
the drag. The nose of the airplane must be pitched down using the elevators. The amount of
altitude loss during the recovery depends on several variables, including how slow the airplane is
flying and how quickly the airplane is pitched down. Section 2.6.3.1 of the Airplane Upset
Recovery Training Aid states, “to recover from a stall, angle of attack must be reduced below the
stalling angle—apply nose down pitch control and maintain it until stall recovery.”
Current air carrier training emphasizes the need to maintain altitude through the use of
power during a stall recovery, and most turbine-powered aircraft can be flown nearly to a stall
and recovered primarily with the application of full power (and pitch control inputs as required
272
The captain’s stall training at GIA was consistent with the training that he received at Colgan. The BE-1900
AFM contained a warning to avoid the pitch excursions that can happen as power is increased during an approach-
to-stall recovery. The stall profiles for the clean, takeoff, and landing configurations included the following
comment: “With stall warning indication the aircraft will have approximately 10° nose up pitch. During recovery
DO NOT lower or allow the nose to fall. Allow the aircraft to fly out of the stall.”

NTSB Aircraft Accident Report
127
to counter any power-induced pitch changes). Colgan Q400 pilots indicated that, with approach-
to-stall recoveries, the application of full power would typically require some nose-down
pressure on the control column but that little change in pitch was required. The pilots stated that
they were trained to use a balance of forward and aft column pressure to obtain the desired pitch
during a recovery (rather than use a pronounced push forward) so that the airplane could regain a
flying AOA and airspeed.
273
Even though air carrier pilots are trained to use power to maintain altitude during
approach-to-stall recoveries, positive nose-down control force is the necessary first step that a
pilot must take once an actual aerodynamic stall has occurred. Because the application of power
by itself will not recover a stalled airplane, approach-to-stall training may negatively affect a
pilot’s actions if a full stall were to develop. Although the accident captain responded as trained
when he applied power in an apparent attempt to maintain altitude, he did not apply full power
(the engine power levers were advanced to about 70°, but the rating detent was 80°), and he
responded inappropriately to the stall warning by applying back pressure on the control column.
The NTSB identified three possible reasons related to Colgan’s Q400 approach-to-stall
simulator training to explain why he was apparently startled and confused by the stall warning.
First, Colgan’s simulator training did not include the use of the ref speeds switch set to the
increase position. Thus, the training had not prepared the flight crew to recognize the early
activation of the stick shaker as a result of the ref speeds switch being set to the increase
position. Second, the simulator training was performed as a preplanned proficiency maneuver
(the approach-to-stall maneuvers to be performed are well known by pilots in advance of their
training) rather than as a maneuver with an element of surprise. However, a fully developed stall
is an unplanned, emergency situation in which the airplane’s nose must be pushed down to
reduce the AOA. Third, the simulator training was hand flown by pilots. During the accident
flight, the autopilot had been engaged until the onset of the stick shaker, at which time the
autopilot disconnected automatically. Although autopilot disconnect needs to occur for a stall
recovery maneuver to be accomplished, the captain (and the first officer) had not been trained to
experience the sudden transition from automated to manual flight with an active stall warning.
The NTSB has investigated other accidents in which pilots applied inappropriate nose-up
pitch control inputs during an attempted stall recovery. For example, on October 14, 2004,
Pinnacle Airlines flight 3701, a Bombardier CRJ-200, was on a repositioning flight when the
airplane stalled at 41,000 feet. FDR data showed that the flight crew moved the control column
aft after the first stick shaker activation and moved the column aft with increasing magnitude
after three subsequent activations of the stick pusher.
274
273
During Q400 simulator observations, the NTSB found that initial nose-up pitch attitudes of 7° to 10° were
needed to recover from approaches to stalls with a minimal altitude loss compared with the greater nose-down pitch
attitudes that are typically needed for stall recoveries in small trainer-type aircraft with the minimal loss of altitude
appropriate for the airplane.
274
FDR data showed that the stick shaker activated five times and that the stick pusher activated four times.

NTSB Aircraft Accident Report
128
Also, on December 22, 1996, an Airborne Express DC-8-63 was on a postmodification
functional evaluation flight when it crashed in Narrows, Virginia.
275
The flight crew failed to
apply positive nose-down control inputs in response to a stall at 14,000 feet. (The stall protection
system was inoperative during the flight.) After the airplane stalled, the crew applied power to
recover but did not establish nose-down control inputs.
Another such accident involved West Caribbean Airways flight 708, an MD-82, near
Machiques, Venezuela, on August 16, 2005. FDR data showed that the horizontal stabilizer
reached its full nose-up position as the airplane descended from 31,000 feet. The CVR recorded
the aural warning “stall, stall” and the continuous sound of the stick shaker for 1 minute 46
seconds before impact.
276
The NTSB has continued to advocate for flight crew training in the post-stall flight
regime because of multiple accidents in which flight crews did not apply appropriate recovery
procedures. For example, in a letter dated May 7, 2009, the NTSB commented on an NPRM
titled, “Qualification, Service, and Use of Crewmembers and Aircraft Dispatchers,” which
proposed to amend the regulations for training programs for flight and cabin crewmembers and
dispatchers. The NTSB indicated that stall recovery training should go beyond approaches to
stall to include recoveries from a full stall condition and that available flight data from flight
tests, accidents, and incidents should be used to model stall behavior to facilitate training beyond
the initial stall warning.
If the approach-to-stall training that the flight crew received had been properly applied,
then the crew should have recovered the airplane from the stall warning and the pitch excursion.
However, the NTSB concludes that the current air carrier approach-to-stall training did not fully
prepare the flight crew for an unexpected stall in the Q400 and did not address the actions that
are needed to recover from a fully developed stall. Therefore, the NTSB recommends that the
FAA require Part 121, 135, and 91K operators and Part 142 training centers to develop and
conduct training that incorporates stalls that are fully developed; are unexpected; involve
autopilot disengagement; and include airplane-specific features, such as a ref speeds switch.
2.9.1 Stick Pusher Training
The NTSB has investigated prior accidents in which pilots have responded incorrectly to
the stick pusher. As previously indicated, the NTSB found that the flight crew of Pinnacle
Airlines flight 3701 had responded to the stick pusher activations by pulling back on the control
column, which caused the airplane to enter an aerodynamic stall. As a result, the NTSB issued
Safety Recommendation A-07-4, which asked the FAA to do the following:
277
275
During the flight, a stall series was being performed to verify that the airspeeds at which the airplane
experienced stick shaker activation and stall indication were in accordance with precalculated values for the
airplane.
276
The investigation of this accident is being conducted by the Comite de Investigación de Accidentes Aéreos
of Venezuela.
277
The NTSB notes that it issued a related safety recommendation, A-94-173, to the FAA after the United
Express flight 6291 accident. This recommendation is discussed in section 1.18.1.6.

NTSB Aircraft Accident Report
129
Convene a multidisciplinary panel of operational, training, and human factors
specialists to study and submit a report on methods to improve flight crew
familiarity with and response to stick pusher systems, and, if warranted, establish
training requirements for stick pusher-equipped airplanes based on the findings of
this panel.
On April 13, 2007, the FAA stated that it planned to ask the working group that
developed the Airplane Upset Recovery Training Aid to reconvene and develop materials for this
issue. On January 22, 2008, the NTSB classified this recommendation “Open—Acceptable
Response.”
In November 2008, the revised Airplane Upset Recovery Training Aid was published.
However, the revised guidance does not explicitly address the need for, or methods to
accomplish, stick pusher familiarization training. The NTSB is concerned that classroom training
of this important system is incomplete because the training does not familiarize pilots with the
forces associated with stick pusher activation or provide them with experience in learning the
magnitude of the airplane’s pitch response. In addition, the FAA has not taken any other actions
to meet the intent of Safety Recommendation A-07-4.
During the public hearing for this accident, a Bombardier test pilot stated that company
pilots receive a stick pusher demonstration during training because pilots need to see and
experience the tactile feel associated with the pusher’s operation. Also, a NASA research
scientist remarked that such training would help make the stick pusher’s operation “somewhat
less astonishing” if the pusher were to activate during flight, which could help in a situation
similar to the one faced by the accident flight crew. The NTSB recognizes, however, that pusher
familiarization training needs to be done correctly and provided in a context that does not lead to
negative training.
When he flew the Saab 340, the captain received exposure to the stick pusher during
ground checks before the first flight of the day,
278
and, as indicated in section 2.2.3, he might
have received simulator training on the pusher. However, stick pusher training was not
consistently provided to Colgan’s Q400 pilots, and a check airman stated that about 75 percent
of pilots who were shown the pusher in the simulator would try to recover by overriding the
pusher. After the accident, the company implemented stick pusher familiarization training for its
fleets.
The NTSB concludes that the circumstances of this and other accidents in which pilots
have responded incorrectly to the stick pusher demonstrate the continuing need to train pilots on
the actions of the stick pusher during flight and the airplane’s initial response to the pusher.
Therefore, the NTSB recommends that the FAA require all Part 121, 135, and 91K operators of
stick pusher-equipped aircraft to provide their pilots with pusher familiarization simulator
training. In addition, because the Airplane Upset Recovery Training Aid published in 2008 did
not address the intent of Safety Recommendation A-07-4 and no other FAA action has met the
278
First-flight-of-the-day checks are not substitutes for stick pusher familiarization training in a simulator. In
addition, there may be negative transfer during these checks because of a tendency for pilots to hold some pressure
against the pusher.

NTSB Aircraft Accident Report
130
recommendation’s intent, Safety Recommendation A-07-4 is reclassified “Closed—
Unacceptable Action/Superseded.”
2.9.2 Simulator Fidelity
Flight training simulators contain computer-coded aerodynamic, engine, flight control,
and other models to calculate the forces and moments on the airplane, which are then used to
simulate the airplane’s motion. The FAA’s acceptance of flight training simulator devices had
been guided by AC 120-40B, “Airplane Simulator Qualification,” until May 30, 2008, when
14 CFR Part 60 became effective. Part 60 governs the initial and continuing qualification and use
of flight simulation training devices and outlines the maneuvers and the tolerances to be used
when comparing simulators and flight test time history data. According to Part 60, approval of
full flight simulators (levels A through D) depends on passing a series of objective tests that
compare the response of the simulator with the response of an airplane during a flight test.
Part 60 applies more rigorous standards for all flight simulators than those described in
AC 120-40B. For example, the regulation requires that full flight simulator stall characteristics
be tested “for full stall and initiation of recovery.” One of the simulator tests, “Stall
Characteristics,” states the following requirement, which must be met during the second segment
climb, approach, or landing configuration:
Time histories data must be recorded for full stall and initiation of recovery. The
stall warning signal must occur in the proper relation to buffet/stall … FFSs [full
flight simulators] of airplanes exhibiting a sudden pitch attitude change or ‘g
break’ must demonstrate this characteristic.
The NTSB notes that the stall fidelity testing required under Part 60 is a significant
improvement compared with the testing under AC 120-40B, which required only that the stall
warning signal occur in the proper relation to stall. However, the NTSB also notes that Part 60
contains no bank tolerance requirement for speeds below stick shaker, no pitch tolerance
requirement for any speed, and no requirements to address power-on or turning flight stalls.
279
In
addition, because Part 60 applies only to simulators qualified after May 30, 2008, most training
simulators currently in operation may not meet the regulation’s requirements.
Flight crew training on full stalls and recoveries had not previously been included in
simulator training partly because of industry concerns about the lack of simulator aerodynamic
model fidelity in the post-stall flight regime. However, the NTSB believes that advances in
technology can allow post-stall aircraft behavior to be modeled in simulators.
In the late 1990s, a government/industry commercial aviation safety team found that loss
of control was among the top three causes of all worldwide fatal commercial aircraft accidents
and was the second highest cause of passenger fatalities between 1988 and 1997. In its final
279
The Part 60 requirements for stall characteristics are based on idle power, wings-level stalls at deceleration
entry rates of 1 knot or less per second.
NTSB Aircraft Accident Report
131
report, the team identified several intervention strategies to reduce loss-of-control accidents,
280
including the following:
To mandate stall recognition and recovery training, regulators must modify the
appropriate regulations.
Airlines/operators should develop and implement a ground school and simulator
training program to train pilots to handle post stall recovery as part of advanced
maneuver training.
Regulators should mandate the implementation of a ground school and simulator
training program to train pilots to handle post stall recovery as part of advanced
maneuver training.
The team’s final report also noted, “several of the interventions address the need for
upset recovery, stall and post-stall recovery training. To accomplish this training, improved
aerodynamic modeling near the limits of the flight envelope (high angles of attack and/or
sideslip)
[ ]281
is necessary for appropriate simulator fidelity.”
In response to this work, NASA, along with Boeing, conducted a study beginning in the
late 1990s to increase simulator model fidelity beyond the data envelope that existed at the time.
This study used rotary balance and conventional wind tunnels to develop an aerodynamic model
for the higher AOA and sideslip ranges that are required to simulate stall upsets in large
transport-category airplanes. This enhanced upset recovery aerodynamic model was validated
using certification flight test maneuver data, including stalls, and accident data. NASA and
Boeing reported that simulations involving the enhanced upset recovery aerodynamic model
were able to reasonably reproduce the results of stall flight tests, unlike the baseline simulation
used in flight training at the time.
According to a 2005 paper that summarized findings from the NASA and Boeing study,
this research demonstrated that simulation fidelity could be significantly improved and that the
useful data envelope for upset training could be expanded. The paper concluded, “results from
NASA/Boeing research conducted to date have led to a recommendation to re-examine the
potential uses of simulators that are specifically designed for upset training. This research has
demonstrated that simulation fidelity can be significantly improved such that the useful envelope
for upset training may be expanded.”
282
Similarly, a 2009 paper on aerodynamic modeling for upset training concluded the
following:
280
Joint Safety Analysis Team, Loss of Control, Commercial Aviation Safety Team Approved Final Report,
December 15, 2000.
281
Sideslip is the lateral angle between the longitudinal axis of the airplane and the direction of motion
(flightpath or relative wind). Sideslip is normally produced by rudder forces, yawing motion resulting from
asymmetrical thrust, or lateral gusts.
282
J.V. Foster, K. Cunningham, et al., “Dynamics Modeling and Simulation of Large Transport Airplanes in
Upset Conditions,” American Institute of Aeronautics and Astronautics, Report No. AIAA-2005-5933, 2005.
NTSB Aircraft Accident Report
132
Much work has been performed in the modeling and simulation of flight
dynamics in ‘extreme’ conditions. Through this work, a process has been
established that yields [a] model that [has] very good predictive capability and
subsequent correlation with flight test data. Although most of the work in this
area has focused on highly maneuverable military aircraft, the concepts for data
collection and reduction are well suited for use in the civil arena, as was proven
during two effort[s] sponsored by NASA in the past decade.
283
In June 2009, the Royal Aeronautical Society
284
hosted a flight simulation conference,
titled “Flight Simulation: Towards the Edge of the Envelope.” Participants at the conference
discussed the need for upset recovery training, training strategies, the role of motion cues in
upset recovery training,
285
and aerodynamic modeling for upset recovery training. The
aerodynamic modeling presentations indicated that extended envelope modeling (higher AOA
and sideslip data ranges) was now possible for civil aircraft simulators and pointed out that
military aircraft simulators already included such modeling.
286
Also, a paper presented at the flight simulator conference indicated that Boeing was
testing a higher-data-range simulator that incorporated lessons learned from the NASA and
Boeing study.
287
According to the paper, several pilots who were tested in this higher-data-range
simulator were typically able to complete upset training maneuvers without exceeding the
simulator’s validated flight envelope. Boeing’s testing, however, did not evaluate pilot
performance in upset recoveries with fully developed stall scenarios.
The NTSB notes that among the contributing causes to the Airborne Express/Narrows
accident (previously discussed in section 2.9) was the company’s DC-8 flight training
simulator’s inadequate fidelity in reproducing the airplane’s stall characteristics. Specifically, the
stalls practiced by the flight crew in the training simulator resulted in a high sink rate at a nose-
high attitude without the large roll excursions and uncommanded pitch-down experienced by the
accident airplane. As a result, on July 29, 1997, the NTSB issued Safety Recommendation
A-97-47, which asked the FAA to do the following:
Evaluate the data available in the stall characteristics of airplanes used in air
carrier service and, if appropriate, require the manufacturers and operators of
flight simulators used in air carrier pilot training to improve the fidelity of these
283
D.R. Gingras and J.N. Ralston, “Aerodynamic Modeling for Training on the Edge,” Proceedings of the
Spring 2009 Flight Simulation Conference, Royal Aeronautical Society, 2009.
284
According to its website, the Royal Aeronautical Society, headquartered in London, England, is a
multidisciplinary professional institution dedicated to the global aerospace community.
285
Higher-level flight simulators consist of a simulated cab on a motion platform to provide pilots with onset
motion cues. Such cues provide a vestibular/kinetic sense of the aircraft’s motion, which is coupled with the motion
of the visual scene.
286
As a result of the conference, the Royal Aeronautical Society chartered an international committee for
aviation training in extended flight envelopes. The committee’s goals are to define best practices for upset recovery,
training scenarios for these best upset recovery practices, and methods to validate simulator responses in training
these scenarios.
287
David C. Carbaugh, Robert A. Curnutt, et al., “Simulator Upset Recovery Training,” Proceedings of the
Spring 2009 Flight Simulation Conference, Royal Aeronautical Society, 2009.

NTSB Aircraft Accident Report
133
simulators in reproducing the stall characteristics of the airplanes they represent
to the maximum extent that is practical; then add training in recovery from stalls
with pitch attitudes at or below the horizon to the special events training programs
of air carriers.
On June 9, 1999, the FAA stated that an aircraft in an aerodynamic stall might handle and
perform differently than the programming in the simulator might indicate for an identical
circumstance and that the acquisition of data in this flight condition would have questionable
accuracy and would be costly and dangerous to acquire. On November 19, 1999, the NTSB
stated that the ability of simulators to replicate an airplane’s actions in some stall and stall
recovery regimes could be improved and that the FAA’s lack of action to improve simulator
fidelity in reproducing stall characteristics was disappointing. As a result, Safety
Recommendation A-97-47 was classified “Closed—Unacceptable Action.”
As previously discussed, advances in post-stall modeling have occurred since the FAA’s
June 1999 response to Safety Recommendation A-97-47. However, during this and other
accidents (including the Airborne Express/Narrows and the West Caribbean Airways flight 708
accidents), the pilots did not apply appropriate recovery controls after the airplane entered a
sustained stall,
288
and the AOA might have exceeded the AOA validated for the full stall and
initiation of recovery required by Part 60. In addition, statistics from the government/industry
commercial aviation safety team for 1999 through 2008 showed that loss of control had become
the leading cause of all worldwide fatal commercial aircraft accidents and the leading cause of
passenger fatalities.
Operators should be aware of the possibility of negative effects when conducting stall
training in flight regimes that exceed the validated flight envelope. If the full stall training
requested in Safety Recommendation A-10-22 would be accomplished in a simulator, then it is
essential that the simulator be approved for this training beyond the fully developed stall AOA.
Simulator improvements to the high AOA flight characteristics will reduce the likelihood of
negative training. The NTSB concludes that pilots could have a better understanding of an
airplane’s flight characteristics during the post-stall flight regime if realistic, fully developed
stall models were incorporated into simulators that are approved for such training. Therefore, the
NTSB recommends that the FAA define and codify minimum simulator model fidelity
requirements to support an expanded set of stall recovery training requirements, including
recovery from stalls that are fully developed. These simulator fidelity requirements should
address areas such as required AOA and sideslip angle ranges, motion cueing, proof-of-match
with post-stall flight test data, and warnings to indicate when the simulator flight envelope has
been exceeded.
288
During a sustained stall, the airplane can reach AOAs beyond those that occur when an appropriate and a
timely stall recovery technique is used. The flight characteristics of such sustained stalls are different from those of
an unstalled airplane. Timely recognition of sustained stall characteristics could represent the last chance for a pilot
to lower the AOA and recover the airplane.

NTSB Aircraft Accident Report
2.9.3 Tailplane Stall Training
The accident flight crew had seen a NASA-produced video, titled “Icing for Regional and
Corporate Pilots,” during winter operations training in initial, transition, and recurrent ground
school. The video was intended to enhance a pilot’s ability to assess hazardous icing conditions
and understanding of icing effects on an airplane. The video also discussed tailplane stalls and
wing stalls as a result of icing conditions. In addition, the video stated that pilots needed to
properly diagnose icing problems (while maintaining airspeed awareness) because the
differences between a wing and a tailplane stall were subtle but the recovery techniques were
different.
As previously indicated in section 2.2.3.1, the video indicated that tailplane stalls were
most likely to occur with ice accumulation on the horizontal stabilizer and that symptoms of
tailplane stalls included lightening of the controls, pitch excursions, difficulty in pitch trim,
buffeting of the controls, and sudden nose-down pitching. The tailplane stall recovery procedure
discussed in the video required pilots to pull back on the control column; reduce flap setting;
and, for some aircraft, reduce power. However, the tailplane stall recovery procedure presented
in the video was the opposite of the recovery procedure for a conventional wing stall, which
requires lowering the nose and adding power.
Postaccident interviews with Colgan pilots about tailplane stalls produced varying
responses. One captain stated that the video about tailplane icing made a big impression on him,
and another captain stated that the video got his attention. Some pilots indicated that they would
apply the tailplane stall procedure if they had clearly identified the symptoms of a tailplane stall,
whereas other pilots stated that it would be difficult to determine if the airplane was in a
conventional wing stall or a tailplane stall. Some pilots thought that the Q400 might be
susceptible to a tailplane stall, some pilots were not sure about the airplane’s susceptibility, and
one pilot (a check airman) stated that the possibility of a tailplane stall in the Q400 had “never
crossed [his] mind.”
Colgan’s manuals and training materials (except for the NASA icing video) made no
reference to tailplane stalls or tailplane stall recovery techniques. Further, the company’s director
of flight standards indicated that the company did not teach pilots tailplane stall recovery
techniques, and no procedures for tailplane stalls were included in the company’s CFM or the
Q400 AFM.
During the public hearing for this accident, officials from Bombardier testified that the
Q400 was not susceptible to tailplane stalls. For example, the Bombardier principal engineering
test pilot for the DHC-8 series stated that, during Q400 testing, the airplane showed no tailplane
stall tendencies, and a Bombardier engineering manager stated that the company did not have a
tailplane stall recovery procedure because the airplane was demonstrated to be free from
tailplane stalls under all conditions. The engineering manager also stated that he was not aware
of any formal document to Q400 operators indicating that the airplane was not susceptible to
tailplane stalls.
Also during public hearing testimony, the FAA’s manager of air carrier training stated his
belief that no airplanes currently being operated by Part 121 air carriers were susceptible to
134

NTSB Aircraft Accident Report
135
tailplane stalls. He recalled that the early versions of two airplanes, the Saab 340 and the
Jetstream J31, had tailplane stall tendencies but stated that these tendencies were corrected by
airworthiness directives and manufacturing changes. The FAA manager further indicated that
training programs should not lead to negative training or possible miscues regarding how flight
crews are to handle a full wing stall.
As stated in section 2.2.3.1, it is unlikely that the captain was deliberately attempting to
perform a tailplane stall recovery in response to the stick shaker activation. Nevertheless, the
NTSB concludes that the inclusion of the NASA icing video in Colgan Air’s winter operations
training may lead pilots to assume that a tailplane stall might be possible in the Q400, resulting
in negative training. Therefore, the NTSB recommends that the FAA identify which airplanes
operated under Part 121, 135, and 91K are susceptible to tailplane stalls and then (1) require
operators of those airplanes to provide an appropriate airplane-specific tailplane stall recovery
procedure in their training manuals and company procedures and (2) direct operators of those
airplanes that are not susceptible to tailplane stalls to ensure that training and company guidance
for the airplanes explicitly states this lack of susceptibility and contains no references to tailplane
stall recovery procedures.
2.10 Federal Aviation Administration Oversight
Oversight of the Colgan certificate and the Q400 program were provided by a POI and a
Q400 APM. The POI was based at the Washington FSDO, which was near the company’s
headquarters at the time of the accident, and the Q400 APM was based at the Teterboro FSDO,
which was near the EWR base. The investigation of this accident found that FAA records of
oversight activities at Colgan showed no deficiencies related directly to the circumstances of the
accident.
The investigation also found that, between February 2007 and February 2008, Colgan
underwent a period of substantial growth. During this time, the Q400 was introduced into the
company’s operations, a relatively large number of pilots (“a couple of hundred,” according to
the company’s vice president of administration) was hired, and a new Q400 base of operations
was established at EWR.
289
In addition, Colgan had to outsource Q400 flight crew training (with
FlightSafety International in Toronto) until the company could become fully qualified to conduct
its own Q400 flight crew training (which occurred in July 2008).
FAA Order 8900.1, “Flight Standards Information Management System,” notes that POIs
must determine when surveillance retargeting is required based on, among other things,
significant changes in an air carrier’s operating environment, including changes in the scope and
scale of operations (that is, growth or downsizing).
290
The order indicated that such changes
could affect a carrier’s ability to balance its resources, size, and organizational structure with
289
The 15 Q400 airplanes that Colgan purchased and the pilots hired to fly the airplanes represented about a
30-percent increase in the size of the company.
290
FAA Order 8900.1 also states that surveillance retargeting is required for other triggering events, such as
accidents or incidents.
NTSB Aircraft Accident Report
136
operational requirements. The investigation of this accident did not find any evidence that
surveillance retargeting had occurred. For example, no evidence showed that the size of the
certificate management team changed despite the significant growth that Colgan was
experiencing. The POI stated, during a postaccident interview, that the only other aviation safety
inspector on his staff (besides the Q400 APM) was an APM for the Saab 340.
Also, neither the POI nor the previous Q400 APM (who was in the position from March
2007 to February 2008) was qualified on the Q400 at the time that it was initially incorporated
into Colgan’s fleet. The POI received his Q400 training in October and November 2007, which
was the same time that Colgan line pilots were being initially trained on the airplane. Also, he
and the previous APM were responsible for overseeing proving flights
291
for the Q400, even
though they were not completely familiar with the airplane. The current Q400 APM was
assigned to the certificate in March 2008, after Q400 revenue service had begun, and received
his Q400 training in May 2008. Although both FAA aviation safety inspectors were experienced
pilots,
292
they were responsible for overseeing the newly introduced service of an airplane for
which they were not previously qualified and had not flown except during simulator training. As
a result, the inspectors had to continue to become familiar with the airplane while they were
conducting their day-to-day management of the certificate.
In December 2009, Colgan moved its headquarters from the Washington, D.C., area to
Memphis, but the Colgan certificate remained with the Washington FSDO. Thus, the POI is
providing oversight of operations at Colgan headquarters and the company’s training center (also
located in Memphis) from a remote location. However, during its investigation of the December
2007 Air Wisconsin Airlines flight 3758 accident in Providence, Rhode Island, the NTSB found
that providing remote oversight was difficult for the company’s POI, assistant POI, and APM,
who were not located near the company’s primary training center and crew bases.
293
FAA Order 8900.1 also states that rapid expansion or growth of an air carrier could affect
its training programs. In October 2007, during Colgan’s rapid growth period, the captain was
disapproved for a Saab 340 airline transport pilot certificate and type rating on his initial attempt
to upgrade to captain. (He received the airline transport pilot certificate and type rating later that
month on a subsequent attempt.) This disapproval was the captain’s second failed checkride
since beginning work for Colgan; he had also been previously graded “train to proficiency”
during another checkride. Because of his continued weaknesses in basic aircraft control and
attitude instrument flying, the captain was a candidate for remedial training. However, the POI
did not recommend that the company provide remedial or another type of supplemental training
to the captain or other pilots with persistent training deficiencies, even though SAFO 06015,
291
Before revenue service can be operated, proving flights have to be conducted as part of compliance with a
new aircraft process document, which directs the activities and provides guidance for aviation safety inspectors
during the addition of a new aircraft make and model to an air carrier’s operations.
292
During postaccident interviews, the POI stated that he was type rated on the Bombardier CRJ-200, the
Jetstream 31, and an early model DHC-8, and the APM stated that he was type rated on the DHC-8 and a variant of
the Dassault Falcon. Both the POI and APM had accumulated more than 8,000 hours total flight time.
293
The inspectors were located in Chicago, Illinois; the company’s primary training center was located in
Charlotte, North Carolina; and the crew bases were in Philadelphia, Pennsylvania, Washington, D.C., and Norfolk.)
Additional information about this accident, NTSB case number DCA08FA018, is available on the NTSB’s website.

NTSB Aircraft Accident Report
137
issued in 2006, recommended the implementation of such training. (During the public hearing
for this accident, the POI for Colgan stated that he was not aware of the SAFO.)
Even though Colgan’s training and checking programs were approved by the FAA, the
FAA aviation safety inspectors could only conduct a small number of the training and checking
events at the airline because of their other responsibilities. As a result, the inspectors had to rely
on company aircrew program designees (under the aircrew designated examiner program) for
airline transport pilot certifications and type ratings and check airmen for proficiency and line
checks. The POI was responsible for operations within the aircrew designated examiner
program, and the Q400 APM supported the POI by providing surveillance of program activities
associated with that specific airplane type. The APM was also responsible for recommending
candidate aircrew program designees to the POI, who made the selections, and for qualifying
each designee in the conduct of airman certification. In addition, the APM was responsible for
overseeing check airmen and ensuring that they maintained high standards when conducting
proficiency and line checks.
FAA Order 8900.1 further states, “air carrier expansion or growth can also raise potential
safety and quality concerns, and influence the likelihood of noncompliance with existing
processes and controls.” Because of the 15 new Q400 airplanes in its inventory, Colgan needed
to upgrade pilots to Q400 captains and train newly hired (and low-time) pilots as Q400 first
officers. This situation warranted additional FAA oversight of Colgan’s check airmen and
aircrew program designees to ensure that training and checking standards were not affected by
pressures to qualify these pilots. The NTSB notes that this focused oversight was also needed
because of the lack of detail in Colgan’s electronic pilot training records and the lack of previous
Part 121 experience of some company Q400 check airmen and aircrew program designees.
294
Available Q400-qualified aviation safety inspectors from all FAA regions and from Part 142
training centers could have augmented the certificate’s inspectors and provided quality assurance
over Colgan’s aircrew program designees.
In addition, the International Air Transport Association (IATA) and the Department of
Defense (DOD) conducted independent audits of Colgan in 2007. Both of the audits contained
findings that necessitated corrective actions by Colgan. The corrective actions taken by Colgan
in response to the audit findings were accepted by IATA in September 2007 and DOD in April
2008. The Colgan POI stated that he was aware of these audits but did not get a copy of the
reports, which prevented him from having a comprehensive understanding of the reports’
findings. For example, the POI believed that IATA’s findings were minor
295
and that a DOD
issue was not within the scope of his responsibilities because it was not mandated by the FAA.
One finding from the audits involved Colgan’s internal evaluation program (IEP),
296
which is not required by FAA regulations. As stated in section 2.7.2, the NTSB found significant
294
After the accident, the NTSB interviewed five company Q400 check airmen and two company Q400
aircrew program designees. The NTSB learned that none of the check airmen or aircrew program designees had any
previous Part 121 experience before their employment with Colgan.
295
The NTSB has made no determination to characterize the audit findings.
296
As stated in AC 120-59, “Air Carrier Internal Evaluation Programs.” IEPs are voluntary self-monitoring and
auditing programs adopted by most Part 121 air carriers.

NTSB Aircraft Accident Report
138
problems with Colgan’s pilot training records. These problems would likely have been prevented
by a sound IEP, which did not exist at the time of the audits and during Colgan’s period of rapid
growth.
297
However, the issues with Colgan’s IEP were subsequently corrected to the
satisfaction of the auditing organizations. Although the NTSB recognizes that the POI needed to
perform his duties in accordance with stated regulations and procedures, use of evaluation tools,
such as these audits, might have alerted him to items that required close review.
On December 20, 1996, the NTSB issued Safety Recommendation A-96-163 as a result
of its investigation of the December 1995 Tower Air flight 41 accident in Jamaica, New York.
Safety Recommendation A-96-163 asked the FAA to do the following:
Develop, by December 31, 1997, standards for enhanced surveillance of air
carriers based on rapid growth, change, complexity, and accident/incident history;
then revise national flight standards surveillance methods, work programs,
staffing standards, and inspector staffing to accomplish the enhanced surveillance
that is identified by the new standards.
On November 24, 2004, the NTSB stated that the FAA had briefed NTSB staff in
March 2004 about programs related to oversight and surveillance of air carriers, including ATOS
and the Surveillance and Evaluation Program.
298
The NTSB indicated that, during this briefing,
the FAA had stated that the risk indicators used by the Surveillance and Evaluation Program for
targeting surveillance resources included rapid growth or expansion, new or major program
changes, complexity of aircraft or new aircraft types, and accident and incident history. Because
the FAA had developed these surveillance standards, the NTSB classified Safety
Recommendation A-96-163 “Closed—Acceptable Action.”
Since that time, the NTSB has investigated several accidents in which inadequate FAA
oversight was a factor and issued several recommendations to address these inadequacies. For
example, Safety Recommendation A-05-8, issued as a result of the Air Sunshine flight 527
accident (see section 1.18.1.8), asked the FAA in part to review the procedures used during its
oversight of the company, including those for the Surveillance and Evaluation Program, to
determine why the inspections failed to ensure that the operational and maintenance issues that
existed at the company were corrected.
299
Colgan’s substantial growth came at a time when the air carrier was transitioning from,
according to the Q400 APM, a “mom and pop,” or startup, airline. Also, the POI for Colgan
stated that the safety culture at the company was “more reactive than I’d like … not quite as
proactive.” As a result, additional resources for enhanced FAA oversight of the certificate were
needed but were not provided. This situation is problematic because, according to a Pinnacle
Airlines third quarter 2009 financial report, 30 additional Q400s have been ordered for Colgan
297
At that time, the program was in its early stages of development.
298
According to the FAA, as part of the Surveillance and Evaluation Program, tools were developed for
principal inspectors to assess the overall risk situation of a carrier, document and analyze their observations, and
refocus the surveillance program toward those areas for which the highest risks were perceived.
299
Safety Recommendation A-05-8 was classified “Closed—Acceptable Action” on August 27, 2009.

NTSB Aircraft Accident Report
139
(15 of which will be delivered beginning in 2010), continuing the company’s expansion and
rapid growth.
A June 2005 report by the Department of Transportation’s Office of Inspector General
found that, at five Part 121 air carriers that were experiencing rapid growth, FAA inspectors
were not able to effectively use oversight systems (ATOS and the Surveillance and Evaluation
Program) to monitor the rapidly occurring changes.
300
The NTSB concludes that the current
FAA surveillance standards for oversight at air carriers undergoing rapid growth and increased
complexity of operations do not guarantee that any challenges encountered by the carriers as a
result of these changes will be appropriately mitigated. Therefore, the NTSB recommends that
the FAA develop more stringent standards for surveillance of Part 121, 135, and 91K operators
that are experiencing rapid growth, increased complexity of operations, accidents and/or
incidents, or other changes that warrant increased oversight, including the following: (1) verify
that inspector staffing is adequate to accomplish the enhanced surveillance that is promulgated
by the new standards, (2) increase staffing for those certificates with insufficient staffing levels,
and (3) augment the inspector staff with available and airplane-type-qualified inspectors from all
FAA regions and Part 142 training centers to provide quality assurance over the operators’
aircrew program designee workforce.
2.11 Company Policies
2.11.1 Flight Operational Quality Assurance
FOQA is a voluntary safety program in which an air carrier collects, deidentifies, and
analyzes actual in-flight data from a QAR or an FDR to identify potential operational risks and
implement corrective actions. According to the FAA, as of October 30, 2009, 19 of the 82 Part
121 certificate holders had FAA-approved FOQA programs.
301
Although Colgan had received
FAA approval for its FOQA implementation and operations plan in October 2008, the FOQA
program was not fully implemented and was not providing useful information at the time of the
accident. The FAA manager for voluntary safety programs reported that FOQA implementation
could take about 1 year and that Colgan’s implementation efforts were hindered by unanticipated
issues affecting the installation of FOQA hardware. In October 2009, Colgan stated that QAR
data analysis was projected to begin by the end of January 2010.
300
Department of Transportation, Safety Oversight of an Air Carrier Industry in Transition, Report Number
AV-2005-062 (Washington, DC: DOT/OIG, 2005).
301
FOQA programs are not required to be approved by the FAA. However, an advantage of having an FAA-
approved FOQA program is participation in the FAA’s Aviation Safety Information Analysis and Sharing (ASIAS)
system. According to the FAA’s director of aviation safety analytical services, ASIAS is a government-industry
partnership that brings together safety information in a protected forum, allowing queries and analysis of multiple
databases. This director stated that, as of July 2009, 21 air carriers with FAA-approved FOQA programs were
participating in ASIAS. Although ASIAS has been used to analyze events such as tail strikes and wrong runway
departures, it has not yet been used to analyze stick shaker or stall warning events.

NTSB Aircraft Accident Report
140
Colgan’s voluntary reporting systems, including ASAP, did not include any reports of
stall warnings. However, it is possible that a stall warning resulting from a mismatch between
the ref speeds switch and the airspeed bugs may be a more common occurrence than currently
realized, given the circumstances of the accident flight and the BTV event. The frequency and
circumstances of stall warnings could be examined as part of a FOQA program because, in
developing FOQA programs, operators select the recorded flight parameters to be analyzed and
one available parameter is the in-flight activation of the stall warning system.
302
Any
information learned from analysis of FOQA program data could result in revised company
procedures, checklists, and training and could be shared with the FAA and others in the aviation
industry.
the two other U.S. operators of the Q400 are both regional
airlines without FOQA programs.
d whether newer aircraft,
including the Q400, were included in FOQA data monitoring efforts.
cess to
implement a FOQA program could be greatly simplified for operators of these airplanes.
Recommendation A-07-11 was classified “Closed—Acceptable
Action” on January 22, 2008.
operators participated in FOQA. The recommendation asked the FAA to “strongly encourage”
Even though Colgan did not have a functioning FOQA program at the time of the
accident, the company might have benefited from other air carriers’ information about the Q400,
including stall warnings. However,
Most of the operators with FOQA programs were established major airlines, which had a
significant amount of data about the operation of the aircraft in their fleet. At the time of the
accident, the FAA made no systematic attempt to determine whether newer or smaller airlines,
including regional airlines, were participating in FOQA programs an
Not all airplanes are capable of supporting a FOQA data recording. Those airplanes that
are currently able to support these recordings are equipped with a data bus that allows
information to be transmitted in digital format from multiple data sensors to QARs. The FAA
has not done a survey of the Part 121 air carrier fleet to determine how many airplanes are QAR
capable. However, operators of those airplanes that are capable of supporting a QAR recording
might still need a supplemental type certificate for a QAR retrofit, which could be expensive and
time-consuming. Some new aircraft have QAR capability already installed, so the pro
On January 23, 2007, the NTSB issued Safety Recommendation A-07-11, which asked
the FAA to strongly encourage and provide assistance to all regional air carriers to implement an
approved ASAP and a FOQA program. As indicated in section 1.18.1.9, on April 13, 2007, the
FAA stated that it took several actions in response to this recommendation, including
participation at Regional Airline Association conferences to increase awareness of ASAP and
FOQA and the issuance of AC 120-92, which identified FOQA as an integral part of an SMS. As
a result of these actions, Safety
Also in its response to Safety Recommendation A-07-11, the FAA recognized that there
was significant participation in ASAP among regional operators but that only a few regional
302
The accident airplane’s FDR recorded stick shaker and stick pusher parameters once every 4 seconds. In
contrast, a QAR might be designed to record hard-target FOQA parameters at higher sample rates to yield a high-
confidence analysis of stall warning events in the Q400 fleet.

NTSB Aircraft Accident Report
regional air carriers to voluntarily implement a FOQA program, yet only three regional airlines
had FOQA programs either planned or underway as of July 2009.
As indicated in AC 120-82, FOQA programs provide objective safety information that
would not otherwise be obtainable. Also, FOQA was established as a worldwide standard by
ICAO in 2005, but U.S. air carriers are not required to conform with this standard because
FOQA is currently a voluntary program. During his December 2009 testimony before the U.S.
Senate, the FAA Administrator stated that he had asked operators without a FOQA program to
implement this program and develop data analysis processes to ensure effective use of program
information. The NTSB concludes that mandatory FOQA programs would enhance flight safety
because all operators would have readily available data to identify operational risks and use in
developing corrective actions. Therefore, the NTSB recommends that FAA require all Part 121,
135, and 91K operators to (1) develop and implement FOQA programs that collect objective
flight data, (2) analyze these data and implement corrective actions to identified systems safety
issues, and (3) share the deidentified aggregate data generated through these analyses with other
interested parties in the aviation industry through appropriate means.
The NTSB recognizes that, as indicated in AC 120-82, FOQA is built upon the
provisions of 49 United States Code 40123 and 14 CFR Part 193, which establish protection of
voluntarily submitted information. The FAA states in AC 120-82 that maintaining confidentiality
of FOQA information among operators is important for providing a cooperative environment.
If
FOQA data were required to be provided to the FAA, these data would no longer fall under the
protections provided by 49 United States Code 40123 and 14 CFR Part 193. The NTSB
concludes that the viability of FOQA programs depends on the confidentiality of the data, which
would currently not be guaranteed if operators were required to implement these programs and
were required to share the data with the FAA. Therefore, the NTSB recommends that the FAA
seek specific statutory and/or regulatory authority to protect data that operators share with the
FAA as part of any FOQA program.
In addition, Colgan had previously proposed including, as part of its FOQA program, a
sample of CVR recordings from routine line operations. The company indicated that the sample
CVR recordings could be used to determine, among other information, how well pilots adhered
to sterile cockpit and standard operating procedures, which could help to prevent accidents. The
company asserted that its use of the CVR for FOQA purposes would ensure pilots’
confidentiality.
The NTSB has recognized the benefits of using flight recorder information for safety
purposes. For example, on October 1, 2009, the NTSB issued Safety Recommendation A-09-99,
which asked helicopter emergency medical services operators to “establish a structured flight
data monitoring program that incorporates routine reviews of all available sources of information
to identify deviations from established norms and procedures and other potential safety issues.”
Aircraft operators would benefit from similar reviews of available safety information sources
that are downloaded as part of a company’s FOQA program. The NTSB concludes that the
systematic monitoring of all available safety data, as part of a flight operational quality assurance
program, could provide operators with objective information regarding the manner in which
flights are conducted and that a periodic review of this information would enhance flight safety
141
NTSB Aircraft Accident Report
142
by assisting operators in detecting and correcting deviations from standard operating procedures.
Therefore, the NTSB recommends that the FAA require Part 121, 135, and 91K operators to (1)
routinely download and analyze all available sources of safety information, as part of their
FOQA program, to identify deviations from established norms and procedures; (2) provide
appropriate protections to ensure the confidentiality of the deidentified aggregate data; and (3)
ensure that this information is used for safety-related and not punitive purposes.
2.11.2 Use of Personal Portable Electronic Devices on the Flight Deck
The NTSB has identified hazards associated with the use of mobile phone technology
(including texting) in rail and highway accidents and has issued recommendations to restrict the
use of this technology by transport operators.
303
Also, in 2008, the NTSB added, to its Most
Wanted List, the need to restrict cellular telephone use by commercial drivers of school buses
and motorcoaches, except in emergencies.
During the taxi phase of the accident flight, the first officer sent a text message on her
personal cell phone about 2113, which was about 5 minutes 30 seconds before ATC cleared the
flight for takeoff. (Evidence indicated that the airplane was not moving at the time that she used
her mobile phone.) However, AC 91.21-1B, “Use of Portable Electronic Devices Aboard
Aircraft,”
304
which was issued on August 25, 2006, indicated that cell phones were not to be
used while an aircraft was taxiing for departure after leaving the gate. The AC further stated that
cell phones should be turned off and properly stored so that the aircraft could be prepared for
takeoff. Although Colgan’s policy on the use of mobile phones on the flight deck was consistent
with the guidance contained in AC 91.21-1B, the company’s pilot checklists did not address
turning off cell phones in preparation for departure. Colgan also stated that it considered the use
of cell phones by flight crewmembers to be covered as part of sterile cockpit procedures.
On February 4, 2009, the FAA published SAFO 09003, “Cellular Phone Usage on the
Flight Deck.” The purpose of this SAFO was to alert all Part 121 and 135 operators to the
potential hazards associated with flight crewmembers leaving their cellular phones on during
critical phases of flight. The SAFO was the result of an inspector’s observation of a ring
tone/warbling sound coming from a first officer’s cellular phone during a takeoff roll just before
reaching the airplane’s takeoff decision speed. The SAFO stated that the ring tone was a
303
For example, on November 30, 2006, the NTSB issued Safety Recommendation H-06-27, which asked the
Federal Motor Carrier Safety Administration to “publish regulations prohibiting cellular telephone use by
commercial driver’s license holders with a passenger-carrying or school bus endorsement, while driving under the
authority of that endorsement, except in emergencies.” The recommendation is currently classified “Open—
Acceptable Response.” Also, on June 13, 2003, the NTSB issued Safety Recommendation R-03-1, which asked the
Federal Railroad Administration to “promulgate new or amended regulations that will control the use of cellular
telephones and similar wireless communication devices by railroad operating employees while on duty so that such
use does not affect operational safety.” The recommendation was classified “Closed—Acceptable Alternate Action”
on September 17, 2009.
304
According to the AC, portable electronic devices are personal devices that include, for example, mobile
telephones; computers with wireless network capabilities; and other wireless-enabled devices, such as personal
digital assistants. Such devices are not provided by an operator for use in supporting flight operations. Electronic
flight bags or laptop computers used for landing performance calculations would thus not be considered personal
portable electronic devices.

NTSB Aircraft Accident Report
143
distraction to the flight crew and could have resulted in an unnecessary rejected takeoff. The
FAA found that the company’s guidance did not prohibit flight crewmembers from leaving
phones on while on the flight deck and that the company’s checklists did not address turning off
cell phones in preparation for departure.
The SAFO recommended that directors of operations of all Part 121 and 135 certificate
holders review guidance to determine if procedures are in place to remind flight crews to turn off
phones while on the flight deck. The SAFO also recommended a review and evaluation of the
operator’s indoctrination and recurrent training curriculums concerning cell phone use and the
sterile cockpit concept.
On October 21, 2009, Northwest Airlines flight 188, an Airbus A320, N374NW, became
a “NORDO” (no radio communications) flight at 37,000 feet. The flight was operating under 14
CFR Part 121 from San Diego, California, to Minneapolis-St. Paul International/Wold-
Chamberlain Airport (MSP) with 5 crewmembers and 144 passengers on board. The flight was
NORDO for about 1 hour 17 minutes. During that time, the airplane flew past MSP and
continued northeast for about 100 miles. When the flight crew and the MSP center controller
reestablished communications, the first officer stated, “we got distracted and we’ve overflown
MSP. We are overhead Eau Claire [Wisconsin] and would like to make a 180 [degree turn] and
do an arrival from Eau Claire.” About 5 minutes later, the controller asked the first officer to
explain what had caused the situation, and he replied, “just cockpit distraction, that’s all I can tell
you.”
During interviews with the Northwest flight crew, the NTSB learned that the distraction
involved the use of personal laptop computers during the discussion of new flight crew
scheduling software and procedures. However, Delta Air Lines policy (which governed
Northwest operations as a result of a merger with the company),
305
prohibited the use of personal
computers and other personal electronic devices on the flight deck.
306
Although the Colgan first officer’s use of her personal cell phone during the taxi phase of
the accident flight was not directly associated with the accident, the event described in SAFO
09003 illustrates the potential for such devices to create a hazardous distraction during a critical
phase of flight. In addition, the Northwest event showed that the use of a personal computer
during cruise flight could severely affect flight crew situational awareness. The NTSB concludes
that distractions caused by personal portable electronic devices affect flight safety because they
can detract from a flight crew’s ability to monitor and cross-check instruments, detect hazards,
and avoid errors. Therefore, the NTSB recommends that the FAA require all Part 121, 135, and
91K operators to incorporate explicit guidance to pilots, including checklist reminders as
appropriate, prohibiting the use of personal portable electronic devices on the flight deck.
305
Delta’s website indicated that the airline had acquired ownership of Northwest and was in the process of
fully integrating Northwest into Delta’s operations.
306
For more information about this incident, see DCA10IA001 on the NTSB’s website.

NTSB Aircraft Accident Report
144
2.12 Safety Alerts for Operators
According to FAA Order 8000.87A, SAFOs “contain important safety information that is
often critical.” SAFOs are intended for FAA inspectors; air carrier directors of safety, operations,
and maintenance; fractional ownership program managers; training center managers; repair
station managers; and others as applicable. Although FAA inspectors are among the intended
audience, the order states, “SAFOs do not burden FAA inspectors with additional responsibilities
not included in their work programs and not processed in accordance with the agreement
between the FAA and its inspectors’ bargaining unit.” At the public hearing for this accident, the
FAA’s manager of air carrier operations asserted that this language was included in the order
because FAA inspectors are heavily tasked.
As previously noted, the FAA had issued SAFOs concerning issues identified in this
investigation, including SAFO 06004, “Approach and Landing Accident Reduction: Sterile
Cockpit, Fatigue,” dated April 28, 2006, and SAFO 06015, “Remedial Training for Part 121
Pilots,” dated October 27, 2006 (see sections 1.18.1.1 and 1.18.1.7, respectively). The
recommended actions discussed in these SAFOs included increased emphasis on sterile cockpit
discipline, fatigue countermeasures and operator fatigue management, and additional training
and oversight for pilots who have experienced multiple training and checking failures. FAA
Order 8000.87A stated that operators are responsible for implementing the actions recommended
in a SAFO. However, no evidence showed that Colgan had initiated any of the recommended
actions in these SAFOs.
The FAA does not routinely track whether the recommended actions included in SAFOs
have been adopted,
307
citing inspector workload as a reason. The FAA order states that SAFOs
are “especially valuable” to air carriers in meeting their statutory duty to operate with the highest
degree of safety. The NTSB recognizes the importance of an air carrier’s statutory responsibility
to provide safe transportation. However, the FAA has a statutory responsibility to provide
effective oversight of the aviation industry. Assessing an operator’s need to implement action on
“important safety information that is often critical” and measuring the resulting change is an
inherent responsibility of FAA inspectors and must be considered part of their workload.
Delegating the responsibility for these actions solely to an operator may not produce the desired
outcome.
SAFOs may be an appropriate method for disseminating routine or initial information to
operators in a timely manner. However, when safety-critical information, which often requires a
change in industry practices or procedures, needs to be distributed, SAFOs are not the
appropriate format because no requirement exists for the FAA to measure whether the SAFO
achieved its intended result. The FAA uses an SMS approach to structure its oversight processes,
but transmitting critical safety information to operators without measuring results is inconsistent
with the basic principles of this system.
307
The FAA has undertaken tracking efforts for some SAFOs to determine whether the desired safety benefit
has been realized. For example, FAA Notice 8900.71 was issued on April 23, 2009, in response to the NTSB’s
March 2009 request for an assessment of industry actions taken in response to SAFOs 06015 and 06005 (the latter
of which discussed bounced landing training).
NTSB Aircraft Accident Report
145
The FAA’s manager of air carrier operations testified at the public hearing that the
agency was considering the establishment of a new transmittal method for safety-critical
information, referred to as an operational directive, which would be similar to an airworthiness
directive. Thus, operators would be responsible for complying with the operational directive, and
FAA inspector surveillance would be required to determine whether the recommended actions
had been accomplished. The NTSB is encouraged that the FAA is considering this new method
for transmitting safety-critical information. The same safety benefit could be achieved if the
FAA revised Order 8000.87A so that the SAFO process would incorporate FAA followup. The
NTSB concludes that the current use of SAFOs to transmit safety-critical information is not
effective because oversight and documentation of an operator’s response are not required and
critical safety issues may not be effectively addressed. Therefore, the NTSB recommends that
the FAA implement a process to document that all Part 121, 135, and 91K operators have taken
appropriate action in response to safety-critical information transmitted through the SAFO
process or another method.
2.13 Preflight Weather Documents and Icing Terminology
As previously stated, no evidence showed that the icing conditions that existed before the
accident were abnormal for wintertime operations in the BUF area. However, the NTSB’s
investigation of this accident identified two weather-related safety issues—preflight weather
documents provided to Part 121 flight crews and icing terminology used in the Aeronautical
Information Manual (AIM)—that warranted changes. These issues are discussed in sections
2.13.1 and 2.13.2, respectively.
2.13.1 Preflight Weather Documents
Chapter 26 of FAA Order 8900.1, Aviation Weather Information Systems for Air
Carriers, section 3-2094, “Operational Requirements—Flightcrews,” states the following
regarding weather information provided to flight crews:
Flightcrews need accurate weather information to determine the present and
forecast weather conditions on any planned operation. For example, for adequate
flight planning, flightcrews should know existing and expected weather
conditions at the departure airport, along the planned route of flight, and at
destination, alternate, and diversionary airports.
The section also provides a list of the numerous weather products that flight crews need
to consider in operational preflight planning decisions.
Chapter 26 of the order, section 3-2096, “Adverse Weather Phenomena Reporting and
Forecasting Requirements,”
308
states that any weather information system used in Part 121
308
According to section 3-2096, adverse weather phenomena are meteorological conditions that could affect
safety if encountered during flight or ground operations. Examples of such phenomena include surface winds
NTSB Aircraft Accident Report
146
operations must include an FAA-approved adverse weather phenomena reporting and forecasting
subsystem. Such subsystems allow operators to monitor weather reports from various sources to
quickly and accurately identify adverse weather phenomena and predict their effects on flight
and ground operation safety. The subsystems are required to include forecasting capabilities that
are at least equal to those of government weather forecasting systems.
309
Even though the
subsystems are automated, dispatch personnel are responsible for (1) programming the
subsystems to ensure that they capture specific weather products during specific time periods for
the arrival and alternate airports for each flight and (2) providing weather documents containing
this information to flight crews. In this case, the Colgan director of dispatch was responsible for
programming the company’s FAA-approved private weather contractor subsystem to capture
specific weather products for the route of flight between EWR and BUF (and from EWR to
ROC, the alternate airport).
The weather document for the accident flight was issued about 1800. The NTSB’s review
of this document revealed that it was missing pertinent information. For example, the weather
document did not contain relevant AIRMETs, even though they are among the in-flight weather
advisories that flight crews need to determine present and forecast weather conditions for an
operation. One of the missing AIRMETs relevant to the accident flight extended over the flight
route and alerted pilots to expect moderate rime icing below 8,000 feet. Another missing and
relevant AIRMET extended over a larger region in the northeast, including the accident site, and
alerted pilots to expect occasional moderate icing below 18,000 feet. The icing conditions in
both of these AIRMETs were expected to last from 2145 to 0400 the next day.
310
The NTSB’s
investigation of this accident verified the conditions detailed in the AIRMETs.
The only icing information included in the weather document for the accident flight was
the reports and forecast of snow at BUF and two PIREPs indicating light-to-moderate rime icing
in the BUF area between 3,000 and 14,000 feet. Even though the minimal aircraft performance
degradation resulting from ice accumulation did not affect the flight crew’s ability to fly and
control the airplane, the NTSB is concerned that pertinent preflight information regarding icing
along the flight route was not relayed to the crew. The AIRMETs relevant to the accident flight
that were not included in the weather document would have provided the crew with additional
information about icing and, accordingly, would have increased situational awareness. However,
this increased situational awareness would not likely have affected the outcome of the flight for
the reasons previously discussed in section 2.2.
On August 15, 1996, the NTSB issued Safety Recommendation A-96-48 as a result of its
investigation of the American Eagle flight 4184 accident in Roselawn, Indiana (see section
exceeding 30 knots, active thunderstorms, moderate or severe in-flight icing, severe or extreme turbulence, and
meteorological conditions causing runway surface contamination.
309
According to 14 CFR 121.101, “each certificate holder conducting domestic or flag operations shall adopt
and put into use an approved system for obtaining forecasts and reports of adverse weather phenomena, such as
clear air turbulence, thunderstorms, and low altitude wind shear, that may affect safety of flight on each route to be
flown and at each airport to be used.”
310
Other AIRMETs in effect at the time described IFR conditions and turbulence over the BUF area. These
AIRMETs were also not included in the weather document.

NTSB Aircraft Accident Report
147
1.18.1.13). Safety Recommendation A-96-48 recognized the importance of AIRMETs and
Center Weather Advisories (CWAs)
311
in flight planning and asked the FAA to do the following:
Direct principal operations inspectors (POIs) to ensure that all 14 Code of Federal
Regulations (CFR) Part 121 air carriers require their dispatchers to provide all
pertinent information, including airman’s meteorological information (AIRMETs)
and Center Weather Advisories (CWAs), to flightcrews for preflight and in-flight
planning purposes.
On April 24, 1997, the FAA stated that it issued Flight Standards Information Bulletin for
Air Transportation 97-03 on March 17, 1997, which directed POIs to ensure that air carriers
require dispatchers to provide pertinent information, including AIRMETs and CWAs, when
appropriate, for preflight and in-flight planning purposes. The FAA also stated that the
information in the bulletin would be incorporated into FAA Order 8400.10, “Air Transportation
Operations Inspector’s Handbook.”
312
On August 20, 1997, the NTSB stated that the flight
standards information bulletin addressed the intent of Safety Recommendation A-96-48 and
classified it “Closed—Acceptable Action.” However, this accident demonstrates that, even
though the FAA took actions to address this safety issue, weather documents are still missing
pertinent information, including AIRMETs.
In addition, the NTSB’s review of the weather document for the accident flight revealed
that some of the information was outdated. For example, the weather document included three
CWAs,
but they were not valid at the time of the accident flight.
313
Also, the wind and temperature
aloft forecast for BUF, which was issued about 1300 and was valid between 1200 and 1600, had
expired before the accident flight. This outdated information should not have been part of the
weather document but was included in it because of programming limitations of Colgan’s
weather contractor subsystem.
Problems with weather documents have also been found at other Part 121 air carriers. For
example, on April 12, 2007, Pinnacle Airlines flight 4712, a Bombardier/Canadair Regional Jet
CL600-2B19, N8905F, departed the end of the runway while landing at Cherry Capital Airport,
Traverse City, Michigan (see section 1.18.1.5). None of the 3 crewmembers and 49 passengers
was injured; the airplane was substantially damaged. The accident flight’s weather document,
which was prepared by the Pinnacle Airlines dispatcher, did not include any NWS in-flight
weather advisories. However, NWS AIRMETs for icing, turbulence, and IFR conditions were
valid for the area at the time of the accident.
Also, on December 25, 2007, Alaska Airlines flight 464, a McDonnell Douglas DC-9-83,
N943AS, encountered severe turbulence during the descent for landing at Ontario International
311
A CWA is an aviation warning for conditions that are meeting or approaching national in-flight advisory
criteria (for example, AIRMETs, SIGMETs, or Convective SIGMETs) and are impacting the respective airspace.
These short-term warnings are typically valid for 2 hours.
312
FAA Order 8400.10 has been superseded by FAA Order 8900.1.
313
Two CWAs for low-level windshear, issued by the New York Air Route Traffic Control Center, had
expired at 1320. A CWA for scattered thunderstorms, issued by the Cleveland Center, expired about 1630.

NTSB Aircraft Accident Report
148
Airport, Ontario, California.
314
Two flight attendants sustained serious injuries during the
turbulence encounter, and the third flight attendant, the two flight crewmembers, and the
109 passengers were not injured. During its investigation of this accident, the NTSB determined
that two NWS Significant Meteorological Information (SIGMET) advisories were not included
in the weather document for the flight. The SIGMETs were issued before the flight’s departure
as a result of occasional severe turbulence for the Ontario area. The NTSB determined the
probable cause of this accident was the lack of turbulence forecast information available to the
flight crew, which resulted in the flight attendants not being seated when the flight encountered
the severe turbulence. Contributing factors to the accident included the failure of the company
that provided the flight’s weather briefing information to forecast severe turbulence and the
failure of the airline dispatcher to provide the SIGMETs to the flight crew.
315
Flight crews need to be provided with an operationally useful weather document
containing all relevant weather information, including AIRMETs and SIGMETs, for each flight
so that they can make sound safety-of-flight decisions based on that information. Such
documents must contain up-to-date information so that flight crews do not have to sort through
outdated or unrelated information for their flight. The NTSB concludes that weather documents
missing key weather products or containing products that are no longer valid prevent flight
crewmembers from having relevant, readily available weather-related safety information for
preflight and in-flight decision-making. Therefore, the NTSB recommends that the FAA require
Part 121, 135, and 91K operators to revise the methodology for programming their adverse
weather phenomena reporting and forecasting subsystems so that the subsystem-generated
weather document for each flight contains all pertinent weather information, including AIRMET,
SIGMET, and other NWS in-flight weather advisories, and omits weather information that is no
longer valid. The NTSB further recommends that the FAA require POIs of Part 121, 135, and
91K operators to periodically review the weather documents generated for their carriers to verify
that those documents are consistent with the information requested in Safety Recommendation
A-10-32.
2.13.2 Icing Terminology
Chapter 7 of the AIM, Safety of Flight, section 7-1-21, describes the effects of ice on an
aircraft and provides terminology for pilots to use when describing icing conditions to ATC.
However, during its investigation of this accident, the NTSB found that the definitions for
reportable icing intensities in the July 2008 version of the AIM had not been updated to reflect
the definitions published in December 2007 in AC 91-74A, “Pilot Guide: Flight in Icing
Conditions.” Table 4 shows the differences in terminology between AIM section 7-1-21(b) and
AC 91-74A.
314
Additional information about this accident, NTSB case number SEA08LA050, is available on the NTSB’s
website.
315
The NTSB discussed these weather-related issues with Alaska Airlines, which added NWS products to the
weather subsystem used to generate its weather documents.
NTSB Aircraft Accident Report
Table 4. Icing Definitions
Icing intensity Aeronautical Information Manual
definition
Advisory Circular 91-74A definition
Trace
Ice becomes perceptible. Rate of
accumulation is slightly greater than
sublimation. Deicing/anti-icing equipment is
not utilized unless encountered for an
extended period of time (over 1 hour).
Ice becomes noticeable. The rate of
accumulation is slightly greater than the rate of
sublimation. A representative accretion rate for
reference purposes is less than 1/4 inch
(6 mm) per hour on the outer wing. The pilot
should consider exiting the icing conditions
before they become worse. Pilots should be
aware that any ice, even in trace amounts,
could be potentially hazardous.
Light
The rate of accumulation may create a
problem if flight is prolonged in this
environment (over 1 hour). Occasional use of
deicing/anti-icing equipment
removes/prevents accumulation. It does not
present a problem if the deicing/anti-icing
equipment is used.
The rate of ice accumulation requires
occasional cycling of manual deicing systems
to minimize ice accretions on the airframe. A
representative accretion rate for reference
purposes is 1/4 inch to 1 inch (0.6 to 2.5 cm)
per hour on the outer wing. The pilot should
consider exiting the condition.
Moderate
The rate of accumulation is such that even
short encounters become potentially
hazardous and use of deicing/anti-icing
equipment or flight diversion is necessary.
The rate of ice accumulation requires frequent
cycling of manual deicing systems to minimize
ice accretions on the airframe. A representative
accretion rate for reference purposes is 1 to 3
inches (2.5 to 7.5 cm) per hour on the outer
wing. The pilot should consider exiting the
condition as soon as possible.
Heavy
None. The rate of ice accumulation requires
maximum use of the ice protection systems to
minimize ice accretions on the airframe. A
representative accretion rate for reference
purposes is more than 3 inches (7.5 cm) per
hour on the outer wing. Consider immediate
exit from the conditions.
Severe
The rate of accumulation is such that
deicing/anti-icing equipment fails to reduce or
control the hazard. Immediate flight diversion
is necessary.
The rate of ice accumulation is such that ice
protection systems fail to remove the
accumulation of ice, and ice accumulates in
locations not normally prone to icing, such as
areas aft of protected surfaces and any other
areas identified by the manufacturer.
Immediate exit from the condition is necessary.
Note: AC 91-74A also states that deicing or anti-icing systems are expected to be activated and operated continuously in the
automatic mode, if available, at the first sign of ice accumulation or as directed in the AFM and that occasional and frequent cycling
refers to manually activated systems. The AC further states that accretion rates can be measured by an icing rate meter.
As shown in table 4, three main differences exist between the icing terminology in the
AIM and AC 91-74A. First, the AC provides an accretion rate for each icing definition, which
can help pilots evaluate and accurately describe the icing conditions. Second, the AC contains a
fifth icing category—heavy—to explain the environment that occurs between moderate and
severe icing, providing additional icing information for pilots to consider. Last, the AC includes
more detailed guidance than the AIM for pilot actions in icing conditions, providing pilots with
further information for addressing specific icing situations.
The light-to-moderate icing terminology used in the two PIREPs that were included in
the weather document for the accident flight had likely portrayed accurate conditions at the time
149

NTSB Aircraft Accident Report
of the flight. Nevertheless, the NTSB is concerned that pilots transmitting airframe icing PIREPs
may not be using the most updated definitions in determining and reporting the severity of icing.
Although the AC is advisory only, it is important that the icing definitions and accretion rates in
the AC be incorporated into the AIM because that publication is the FAA’s official guide for
basic flight information and ATC procedures. The NTSB concludes that detailed icing
definitions that include accretion rates and recommended pilot actions would help pilots more
accurately determine the icing conditions to report in airframe icing PIREPs and more
effectively respond to those conditions. Therefore, the NTSB recommends that the FAA update
the definitions for reportable icing intensities in the AIM so that the definitions are consistent
with the more detailed intensities defined in AC 91-74A.
150

NTSB Aircraft Accident Report
3. Conclusions
3.1 Findings
1. The flight crew was properly certificated and qualified in accordance with applicable Federal
regulations.
2. The airplane was properly certified, equipped, and maintained in accordance with Federal
regulations.
3. The recovered components showed no evidence of any preimpact structural, engine, or
system failures, including no indications of any problems with the airplane’s ice protection
system.
4. The air traffic controllers who were responsible for the flight during its approach to Buffalo-
Niagara International Airport performed their duties properly and responded immediately
and appropriately to the loss of radio and radar contact with the flight.
5. This accident was not survivable.
6. The captain’s inappropriate aft control column inputs in response to the stick shaker caused
the airplane’s wing to stall.
7. The minimal aircraft performance degradation resulting from ice accumulation did not affect
the flight crew’s ability to fly and control the airplane.
8. Explicit cues associated with the impending stick shaker onset, including the decreasing
margin between indicated airspeed and the low-speed cue, the airspeed trend vector pointing
downward into the low-speed cue, the changing color of the numbers on the airplane’s
indicated airspeed display, and the airplane’s excessive nose-up pitch attitude, were
presented on the flight instruments with adequate time for the pilots to initiate corrective
action, but neither pilot responded to the presence of these cues.
9. The reason the captain did not recognize the impending onset of the stick shaker could not be
determined from the available evidence, but the first officer’s tasks at the time the low-speed
cue was visible would have likely reduced opportunities for her timely recognition of the
impending event; the failure of both pilots to detect this situation was the result of a
significant breakdown in their monitoring responsibilities and workload management.
10. The flight crew did not consider the position of the reference speeds switch when the stick
shaker activated.
151

NTSB Aircraft Accident Report
152
11. The captain’s response to stick shaker activation should have been automatic, but his
improper flight control inputs were inconsistent with his training and were instead consistent
with startle and confusion.
12. The captain did not recognize the stick pusher’s action to decrease angle-of-attack as a
proper step in a stall recovery, and his improper flight control inputs to override the stick
pusher exacerbated the situation.
13. It is unlikely that the captain was deliberately attempting to perform a tailplane stall
recovery.
14. No evidence indicated that the Q400 was susceptible to a tailplane stall.
15. Although the reasons the first officer retracted the flaps and suggested raising the gear could
not be determined from the available information, these actions were inconsistent with
company stall recovery procedures and training.
16. The Q400 airspeed indicator lacked low-speed awareness features, such as an amber band
above the low-speed cue or airspeed indications that changed to amber as speed decrease
toward the low-speed cue, which would have facilitated the flight crew’s detection of the
developing low-speed situation.
17. An aural warning in advance of the stick shaker would have provided a redundant cue of the
visual indication of the rising low-speed cue and might have elicited a timely response from
the pilots before the onset of the stick shaker.
18. The captain’s failure to effectively manage the flight (1) enabled conversation that delayed
checklist completion and conflicted with sterile cockpit procedures and (2) created an
environment that impeded timely error detection.
19. The monitoring errors made by the accident flight crew demonstrate the continuing need for
specific pilot training on active monitoring skills.
20. Colgan Air’s standard operating procedures at the time of the accident did not promote
effective monitoring behavior.
21. Specific leadership training for upgrading captains would help standardize and reinforce the
critical command authority skills needed by a pilot-in-command during air carrier operations.
22. Because of the continuing number of accidents involving a breakdown of sterile cockpit
discipline, collaborative action by the Federal Aviation Administration and the aviation
industry to promptly address this issue is warranted.
23. The flight crewmembers’ performance during the flight, including the captain’s deviations
from standard operating procedures and the first officer’s failure to challenge these
deviations, was not consistent with the crew resource management (CRM) training that they
had received or the concepts in the Federal Aviation Administration’s CRM guidance.

NTSB Aircraft Accident Report
24. The pilots’ performance was likely impaired because of fatigue, but the extent of their
impairment and the degree to which it contributed to the performance deficiencies that
occurred during the flight cannot be conclusively determined.
25. All pilots, including those who commute to their home base of operations, have a personal
responsibility to wisely manage their off-duty time and effectively use available rest periods
so that they can arrive for work fit for duty; the accident pilots did not do so by using an
inappropriate facility during their last rest period before the accident flight.
26. Colgan Air did not proactively address the pilot fatigue hazards associated with operations at
a predominantly commuter base.
27. Operators have a responsibility to identify risks associated with commuting, implement
strategies to mitigate these risks, and ensure that their commuting pilots are fit for duty.
28. The first officer’s illness symptoms did not likely affect her performance directly during the
flight.
29. The captain had not established a good foundation of attitude instrument flying skills early in
his career, and his continued weaknesses in basic aircraft control and instrument flying were
not identified and adequately addressed.
30. Remedial training and additional oversight for pilots with training deficiencies and failures
would help ensure that the pilots have mastered the necessary skills for safe flight.
31. Colgan Air’s electronic pilot training records did not contain sufficient detail for the
company or its principal operations inspector to properly analyze the captain’s trend of
unsatisfactory performance.
32. Notices of disapproval need to be considered along with other available information about
pilot applicants so that air carriers can fully identify those pilots who have a history of
unsatisfactory performance.
33. Colgan Air did not use all available sources of information on the flight crew’s qualifications
and previous performance to determine the crew’s suitability for work at the company.
34. Colgan Air’s procedures and training at the time of the accident did not specifically require
flight crews to cross-check the approach speed bug settings in relation to the reference speeds
switch position; such awareness is important because a mismatch between the bugs and the
switch could lead to an early stall warning.
35. The current air carrier approach-to-stall training did not fully prepare the flight crew for an
unexpected stall in the Q400 and did not address the actions that are needed to recover from
a fully developed stall.
36. The circumstances of this and other accidents in which pilots have responded incorrectly to
the stick pusher demonstrate the continuing need to train pilots on the actions of the stick
pusher and the airplane’s initial response to the pusher.
153

NTSB Aircraft Accident Report
37. Pilots could have a better understanding of an airplane’s flight characteristics during the
post-stall flight regime if realistic, fully developed stall models were incorporated into
simulators that are approved for such training.
38. The inclusion of the National Aeronautics and Space Administration icing video in Colgan
Air’s winter operations training may lead pilots to assume that a tailplane stall might be
possible in the Q400, resulting in negative training.
39. The current Federal Aviation Administration surveillance standards for oversight at air
carriers undergoing rapid growth and increased complexity of operations do not guarantee
that any challenges encountered by the carriers as a result of these changes will be
appropriately mitigated.
40. Mandatory flight operational quality assurance programs would enhance flight safety
because all operators would have readily available data to identify operational risks and use
in developing corrective actions.
41. The viability of flight operational quality assurance programs depends on the confidentiality
of the data, which would currently not be guaranteed if operators were required to implement
these programs and were required to share the data with the Federal Aviation Administration.
42. The systematic monitoring of all available safety data, as part of a flight operational quality
assurance program, could provide operators with objective information regarding the manner
in which flights are conducted, and a periodic review of this information would enhance
flight safety by assisting operators in detecting and correcting deviations from standard
operating procedures.
43. Distractions caused by personal portable electronic devices affect flight safety because they
can detract from a flight crew’s ability to monitor and cross-check instruments, detect
hazards, and avoid errors.
44. The current use of safety alerts for operators to transmit safety-critical information is not
effective because oversight and documentation of an operator’s response are not required and
critical safety issues may not be effectively addressed.
45. Weather documents missing key weather products or containing products that are no longer
valid prevent flight crewmembers from having relevant, readily available weather-related
safety information for preflight and in-flight decision-making.
46. Detailed icing definitions that include accretion rates and recommended pilot actions would
help pilots more accurately determine the icing conditions to report in airframe icing pilot
reports and more effectively respond to those conditions.
154

NTSB Aircraft Accident Report
155
3.2 Probable Cause
The National Transportation Safety Board determines that the probable cause of this
accident was the captain’s inappropriate response to the activation of the stick shaker, which led
to an aerodynamic stall from which the airplane did not recover. Contributing to the accident
were (1) the flight crew’s failure to monitor airspeed in relation to the rising position of the low-
speed cue, (2) the flight crew’s failure to adhere to sterile cockpit procedures, (3) the captain’s
failure to effectively manage the flight, and (4) Colgan Air’s inadequate procedures for airspeed
selection and management during approaches in icing conditions.

NTSB Aircraft Accident Report
4. Recommendations
4.1 New Recommendations
As a result of the investigation of this accident, the National Transportation Safety Board
makes the following recommendations to the Federal Aviation Administration:
Require 14 Code of Federal Regulations Part 121, 135, and 91K operators to
review their standard operating procedures to verify that they are consistent with
the flight crew monitoring techniques described in Advisory Circular
(AC) 120-71A, “Standard Operating Procedures for Flight Deck Crewmembers”;
if the procedures are found not to be consistent, revise the procedures according
to the AC guidance to promote effective monitoring. (A-10-10)
Require that airspeed indicator display systems on all aircraft certified under
14 Code of Federal Regulations Part 25 and equipped with electronic flight
instrument systems depict a yellow/amber cautionary band above the low-speed
cue or airspeed indicator digits that change from white to yellow/amber as the
airspeed approaches the low-speed cue, consistent with Advisory
Circular 25-11A, “Electronic Flight Displays.” (A-10-11)
For all airplanes engaged in commercial operations under 14 Code of Federal
Regulations Parts 121, 135, and 91K, require the installation of low-airspeed alert
systems that provide pilots with redundant aural and visual warnings of an
impending hazardous low-speed condition. (A-10-12) (Supersedes Safety
Recommendations A-03-53 and -54 and is classified “Open—Unacceptable
Response”)
Issue an advisory circular with guidance on leadership training for upgrading
captains at 14 Code of Federal Regulations Part 121, 135, and 91K operators,
including methods and techniques for effective leadership; professional standards
of conduct; strategies for briefing and debriefing; reinforcement and correction
skills; and other knowledge, skills, and abilities that are critical for air carrier
operations. (A-10-13)
Require all 14 Code of Federal Regulations Part 121, 135, and 91K operators to
provide a specific course on leadership training to their upgrading captains that is
consistent with the advisory circular requested in Safety Recommendation
A-10-13. (A-10-14)
Develop, and distribute to all pilots, multimedia guidance materials on
professionalism in aircraft operations that contain standards of performance for
professionalism; best practices for sterile cockpit adherence; techniques for
156

NTSB Aircraft Accident Report
assessing and correcting pilot deviations; examples and scenarios; and a detailed
review of accidents involving breakdowns in sterile cockpit and other procedures,
including this accident. Obtain the input of operators and air carrier and general
aviation pilot groups in the development and distribution of these guidance
materials. (A-10-15) (Supersedes Safety Recommendation A-07-8)
Require all 14 Code of Federal Regulations Part 121, 135, and 91K operators to
address fatigue risks associated with commuting, including identifying pilots who
commute, establishing policy and guidance to mitigate fatigue risks for
commuting pilots, using scheduling practices to minimize opportunities for
fatigue in commuting pilots, and developing or identifying rest facilities for
commuting pilots. (A-10-16)
Require 14 Code of Federal Regulations Part 121, 135, and 91K operators to
document and retain electronic and/or paper records of pilot training and checking
events in sufficient detail so that the carrier and its principal operations inspector
can fully assess a pilot’s entire training performance. (A-10-17)
Require 14 Code of Federal Regulations Part 121, 135, and 91K operators to
include the training records requested in Safety Recommendation A-10-17 as part
of the remedial training program requested in Safety Recommendation A-05-14.
(A-10-18)
Require 14 Code of Federal Regulations Part 121, 135, and 91K operators to
provide the training records requested in Safety Recommendation A-10-17 to
hiring employers to fulfill their requirement under the Pilot Records Improvement
Act. (A-10-19)
Develop a process for verifying, validating, auditing, and amending pilot training
records at 14 Code of Federal Regulations Part 121, 135, and 91K operators to
guarantee the accuracy and completeness of the records. (A-10-20)
Direct 14 Code of Federal Regulations Part 121, 135, and 91K operators of
airplanes equipped with a reference speeds switch or similar device to (1) develop
procedures to establish that, during approach and landing, airspeed reference bugs
are always matched to the position of the switch and (2) implement specific
training to ensure that pilots demonstrate proficiency in this area. (A-10-21)
Require 14 Code of Federal Regulations Part 121, 135, and 91K operators and
14 Code of Federal Regulations Part 142 training centers to develop and conduct
training that incorporates stalls that are fully developed; are unexpected; involve
autopilot disengagement; and include airplane-specific features, such as a
reference speeds switch. (A-10-22)
Require all 14 Code of Federal Regulations Part 121, 135, and 91K operators of
stick pusher-equipped aircraft to provide their pilots with pusher familiarization
simulator training. (A-10-23) (Supersedes Safety Recommendation A-07-4)
157

NTSB Aircraft Accident Report
Define and codify minimum simulator model fidelity requirements to support an
expanded set of stall recovery training requirements, including recovery from
stalls that are fully developed. These simulator fidelity requirements should
address areas such as required angle-of-attack and sideslip angle ranges, motion
cueing, proof-of-match with post-stall flight test data, and warnings to indicate
when the simulator flight envelope has been exceeded. (A-10-24)
Identify which airplanes operated under 14 Code of Federal Regulations Part 121,
135, and 91K are susceptible to tailplane stalls and then (1) require operators of
those airplanes to provide an appropriate airplane-specific tailplane stall recovery
procedure in their training manuals and company procedures and (2) direct
operators of those airplanes that are not susceptible to tailplane stalls to ensure
that training and company guidance for the airplanes explicitly states this lack of
susceptibility and contains no references to tailplane stall recovery procedures.
(A-10-25)
Develop more stringent standards for surveillance of 14 Code of Federal
Regulations (CFR) Part 121 135, and 91K operators that are experiencing rapid
growth, increased complexity of operations, accidents and/or incidents, or other
changes that warrant increased oversight, including the following: (1) verify that
inspector staffing is adequate to accomplish the enhanced surveillance that is
promulgated by the new standards, (2) increase staffing for those certificates with
insufficient staffing levels, and (3) augment the inspector staff with available and
airplane-type-qualified inspectors from all Federal Aviation Administration
regions and 14 CFR Part 142 training centers to provide quality assurance over
the operators’ aircrew program designee workforce. (A-10-26)
Require all 14 Code of Federal Regulations Part 121, 135, and 91K operators to
(1) develop and implement flight operational quality assurance programs that
collect objective flight data, (2) analyze these data and implement corrective
actions to identified systems safety issues, and (3) share the deidentified
aggregate data generated through these analyses with other interested parties in
the aviation industry through appropriate means. (A-10-27)
Seek specific statutory and/or regulatory authority to protect data that operators
share with the Federal Aviation Administration as part of any flight operational
quality assurance program. (A-10-28)
Require 14 Code of Federal Regulations Part 121, 135, and 91K operators to
(1) routinely download and analyze all available sources of safety information, as
part of their flight operational quality assurance program, to identify deviations
from established norms and procedures; (2) provide appropriate protections to
ensure the confidentiality of the deidentified aggregate data; and (3) ensure that
this information is used for safety-related and not punitive purposes. (A-10-29)
Require 14 Code of Federal Regulations Part 121, 135, and 91K operators to
incorporate explicit guidance to pilots, including checklist reminders as
158

NTSB Aircraft Accident Report
appropriate, prohibiting the use of personal portable electronic devices on the
flight deck. (A-10-30)
Implement a process to document that all 14 Code of Federal Regulations
Part 121, 135, and 91K operators have taken appropriate action in response to
safety-critical information transmitted through the safety alert for operators
process or another method. (A-10-31)
Require 14 Code of Federal Regulations Part 121, 135, and 91K operators to
revise the methodology for programming their adverse weather phenomena
reporting and forecasting subsystems so that the subsystem-generated weather
document for each flight contains all pertinent weather information, including
Airmen’s Meteorological Information, Significant Meteorological Information,
and other National Weather Service in-flight weather advisories, and omits
weather information that is no longer valid. (A-10-32)
Require principal operations inspectors of 14 Code of Federal Regulations
Part 121, 135, and 91K operators to periodically review the weather documents
generated for their carriers to verify that those documents are consistent with the
information requested in Safety Recommendation A-10-32. (A-10-33)
Update the definitions for reportable icing intensities in the Aeronautical
Information Manual so that the definitions are consistent with the more detailed
intensities defined in Advisory Circular 91-74A, “Pilot Guide: Flight in Icing
Conditions.” (A-10-34)
4.2 Previously Issued Recommendations Reiterated in This Report
The NTSB reiterates the following recommendations to the Federal Aviation
Administration:
Require all Part 121 and 135 air carriers to obtain any notices of disapproval for
flight checks for certificates and ratings for all pilot applicants and evaluate this
information before making a hiring decision. (A-05-1)
Require all 14 Code of Federal Regulations Part 121 air carrier operators to
establish training programs for flight crewmembers who have demonstrated
performance deficiencies or experienced failures in the training environment that
would require a review of their whole performance history at the company and
administer additional oversight and training to ensure that performance
deficiencies are addressed and corrected. (A-05-14)
Require that all pilot training programs be modified to contain modules that teach
and emphasize monitoring skills and workload management and include
opportunities to practice and demonstrate proficiency in these areas. (A-07-13)
159

NTSB Aircraft Accident Report
4.3 Previously Issued Recommendations Reclassified in This Report
Safety Recommendation A-07-13 is reclassified “Open—Unacceptable Response” in
section 2.3.1 of this report.
Safety Recommendations A-03-53 and -54 are reclassified “Closed—Unacceptable
Action/Superseded” in section 2.3.3 of this report. The recommendation is superseded by Safety
Recommendation A-10-12.
Safety Recommendation A-07-8 is reclassified “Closed—Unacceptable
Action/Superseded” in section 2.4.2 of this report. The recommendation is superseded by Safety
Recommendation A-10-15.
Safety Recommendation A-05-1 is reclassified “Open—Unacceptable Response” in
section 2.7.3 of this report.
Safety Recommendation A-07-4 is reclassified “Closed—Unacceptable
Action/Superseded” in section 2.9.1 of this report. The recommendation is superseded by Safety
Recommendation A-10-23.
BY THE NATIONAL TRANSPORTATION SAFETY BOARD
DEBORAH A.P. HERSMAN ROBERT L. SUMWALT
Chairman Member
CHRISTOPHER A. HART
Vice Chairman
Adopted: February 2, 2010
160

NTSB Aircraft Accident Report
161
Board Member Statements
Chairman Hersman, Vice Chairman Hart, and Member Sumwalt filed the following
concurring statements.

Notation 8090A
Chairman Hersman, Concurring:
This accident refocuses much needed attention on many long-standing issues of concern to the Safety
Board – issues such as flight crew monitoring, pilot performance and training, sterile cockpit rules, FAA
oversight, and the use of personal electronic devices, among others. I commend our staff for holding a
public hearing and completing a thorough investigation in advance of the one-year anniversary of the
accident. Their accomplishment was significant and had a tremendous impact on identifying critical
concerns in the aviation industry.
I voted in support of the findings, the probable cause and the recommendations and, along with my
colleagues, supported the adoption of the final report. However, during the public Board meeting, I
submitted a proposal to the Board to amend the probable cause by adding fatigue as a fifth contributing
factor, specifically that the flight crew members’ fatigue contributed to the accident because they did not
obtain adequate rest before reporting to duty. After open discussion, the Board rejected the amendment 2
to 1. While I would have preferred for fatigue to be included in the probable cause, that in no way
diminishes my support for the Board’s final product which I believe advances aviation safety.
Let me explain why I think fatigue, an issue that has been on our Most Wanted List of Transportation
Safety Improvements since its inception in 1990, was a factor in this accident. Numerous accident
investigations, research data and safety studies show that operators, like the flight crew in this accident,
who are on duty but have not obtained adequate rest present an unnecessary risk to the traveling public.
Fatigue results from continuous activity, inadequate rest, sleep loss or nonstandard work schedules. The
effects of fatigue include slowed reaction time, diminished vigilance and attention to detail, errors of
omission, compromised problem solving, reduced motivation, decreased vigor for successful completion
of required tasks and poor communication, and generally results in performance deficiencies like those
present during this accident flight. As we conclude in the accident report, the flight crews’ errors,
including the captain’s inappropriate response to the activation of the stick shaker and the flight crews’
failure to monitor air speed, adhere to sterile cockpit procedures and adequately monitor the flight, were
the causal and contributing factors of this accident. But I also believe that these errors are consistent with
fatigue.
According to the FAA, operator fatigue is one of the most persistent hazards in all travel modes, including
commercial aviation.
1
The Safety Board has examined operator fatigue in its safety studies on flight crew
errors,
2
commuter airlines,
3
and aviation safety in Alaska.
4
In the flight crew study, the Board found that
crews, comprised of captains and first officers whose time since awakening was above the median for
their crew position, made more errors overall. In the study on commuter airline safety, the Board found
that self-reports from commuter airline pilots indicated that most pilots had flown while fatigued. In the
study on aviation in Alaska, the Board concluded that the consecutive, long duty days, permitted by Title
14 Code of Federal Regulations (14 CFR) Part 135.261 for commuter airline and air taxi flight crews
1
Federal Aviation Administration, SAFO 06004; Approach and Landing Accident Reduction: Sterile Cockpit,
Fatigue. 04/28/06.
2
National Transportation Safety Board,1994. A Review of Flightcrew-Involved, Major Accidents of U.S. Air
Carriers, 1978 Through 1990. Safety Study NTSB/SS-94/01.
3
National Transportation Safety Board, 1994. Commuter Airline Safety. Safety Study NTSB/SS-94/02.
4
National Transportation Safety Board, 1995. Aviation Safety in Alaska. Safety Study NTSB/SS-95/03.
1

in Alaska, can contribute to fatigue and are a detriment to safety.
5
A 1999 NASA study found that 80% of
regional airline pilots said they had nodded off during a flight,
6
and fatigue continues to show up in
reports in NASA’s Aviation Safety Reporting System.
7
The question is why, after more than 40 years of documentation and investigation of the hazards of
fatigue, so little has changed in our identification of fatigue as a causal or contributing factor in accidents.
I would like to contrast how we have addressed fatigue with two other human factors issues that have
matured in the last four decades -- alcohol impairment and adherence to standard operating procedures
(SOPs).
Today, the impairing effects of alcohol are well understood and accepted by NTSB investigators and
society at-large. However, this has not always been the case. Early in the Safety Board’s history, the
prevailing view was that an individual could be under the influence with a blood alcohol content above
today’s legal limit, and still not be considered drunk. For example, we investigated the 1967 collision in
Baker, California, between a car travelling the wrong way on the highway and a bus which resulted in 20
fatalities and 11 injuries.
8
The NTSB calculated that at the time of the collision, the driver of the car had a
blood-alcohol level of between .15 and .19 (or higher). Nonetheless the accident report states that “there
is a difference between being "under the influence" of alcohol and varying degrees of drunkenness. In the
common acceptance of the term, "drunkenness" is taken to mean that a person is in a helpless state of
immobility.” The report goes on to determine that the driver was not “drunk” because prior to the accident
he successfully traveled around town by car, talked with friends and “therefore, it is logical to believe that
he was able to read, comprehend and respond to traffic control devices, although probably not as well or
as quickly as if he were sober.” In the report, alcohol was not cited as one of the probable cause factors; it
was listed as a contributing factor. The Safety Board concluded that because the driver was not
immobilized by the alcohol, alcohol was not a causal factor. The use of alcohol, to a certain extent, was
tolerated in the transportation industry and by society in general if an impaired individual could still
function at some level.
Fortunately, we have advanced beyond this limited viewpoint. Alcohol testing is now a routine
component of our accident investigations, and society has placed stricter limits on alcohol use. Today,
safety-sensitive transportation employees are subject to random and post-accident drug and alcohol
testing, and every state now has impaired driving laws with an .08 or higher breath or blood concentration
legal limit. Federal regulations establish an even lower .04 limit for transportation professionals.
Fatigue-impaired performance is not unlike alcohol-impaired performance. For example, a 2003 study
demonstrated that sleep loss is at least as potent as ethanol in its performance-impairing effects and two
hours of sleep loss equates to a breath ethanol concentration of approximately .05%.
9
Other studies
establish that prolonged wakefulness significantly impairs speed and accuracy, hand–eye coordination,
5
Evaluation of U.S. Department of Transportation Efforts in the 1990s to Address Operator Fatigue, NTSB/SR-
99/01, May 1999.
6
Co, E.L, et al. Crew Factors in Flight Operations XI: A survey of fatigue factors in regional airline operations.
NASA/TM report no.199-208799.
7
Michael B. Mann, Deputy Associate Administrator, NASA, Hearing on Pilot Fatigue, Aviation Subcommittee of
the Committee on Transportation and Infrastructure, United States House of Representatives, August 3, 1999.
8
National Transportation Safety Board, Interstate Bus Automobile Collision on Interstate Route 15, Baker,
California, March 7, 1968.
9
Roehrs T; Burduvali E; Bonahoom A et al. Ethanol and sleep loss: a “dose” comparison of impairing effects.
Sleep 2003; 26(8):981-5.
2

decision making, and memory,
10
and one study, in fact, correlates prolonged wakefulness with
impairment, such that being awake for 16 hours is equivalent to a .05 BAC.
11
We have successfully identified the problem of impairment due to alcohol and drugs in the workplace,
and the regulators and industry have devised rules, testing and treatment countermeasures to address the
problem. The challenge we face now is creating an environment in which to identify the impairing effects
of fatigue. Whether it is using predictive scheduling tools, technology such as eye or voice assessment,
administering self tests to quickly assess fatigue or even coming up with a blood test to identify the extent
to which fatigue is affecting an individual’s ability to be vigilant, react quickly and avoid both lapses of
attention and response errors – we need to address this critical problem.
12
Another example of the progress we have made during the Safety Board’s four decades-long
investigations of human factors is adherence to Standard Operating Procedures, such as the sterile cockpit
rule (prohibiting extraneous conversation below 10,000 feet). We have made the connection between
violating the sterile cockpit rule and creating a lax environment in the cockpit that results in crews not
being attentive to the task at hand. Today, for sterile cockpit violations to be cited in the probable cause,
crews do not have to be engaged in a conversation at the time the accident sequence commences; the
conversation just has to be present at some point during the flight.
An example of how far this concept has advanced was brought to my attention a few years ago in a
petition for reconsideration for a 1967 mid-air collision of Piedmont Airlines flight 22, a Boeing 727,
with a twin engine Cessna 310. The 727 was departing Asheville Regional Airport in North Carolina and
the Cessna was on approach to the same airport. All 82 people aboard both aircraft were killed. The
petition for reconsideration raised three points, one of which was that the NTSB report made no mention
of a fire in a cockpit ashtray that preoccupied the Piedmont crew in the final 35 seconds before the
collision. The time that lapsed from take-off to collision was only about 2 minutes and 37 seconds,
however, the final accident report’s only reference to the crew’s recorded cockpit conversation stated that
it was “concerned primarily with the operation of the aircraft and nothing was found of a probative value
to the investigation.” As difficult as it is to believe, the crew’s preoccupation with the fire was not
mentioned in the final report.
We have certainly come a long way. Today, extraneous conversation in the cockpit while under 10,000
feet is an unacceptable safety hazard and has regularly been cited as a causal or contributing accident
factor. Like with fatigue, we do not have a test to demonstrate the degree to which a sterile cockpit
violation affects a crew’s performance. We similarly do not require that any causal or contributing factor
equate to a percentage or share of the cause of an accident. Nonetheless, the Safety Board recognizes that
a sterile cockpit violation can be a contributing factor for an accident, as was the case in this accident. In
this accident, the crew was not behind in their checklists and had not violated the sterile cockpit rule in
the two minutes prior to the upset. However the Board did believe that the sterile cockpit violation earlier
in the flight created an “environment” where errors were not detected or recognized. Consequently, the
sterile cockpit violation was one of four contributing factors to the accident. The exact same logic should
be applied to our determination of fatigue; we can demonstrate that the crew was fatigued at the time of
the accident and consistent with research, data and science, fatigue results in performance deficiencies
that were displayed by the crew. Thus, fatigue should be included as a contributing factor.
10
Babkoff et al., 1988; Florica et al., 1968; Gillberg et al., 1994; Linde and Bergstrom, 1992; Mullaney et al., 1983.
11
Dawson D, Reid K: Fatigue, alcohol and performance impairment. Nature 1997; 388: 235.
12
Fatigue Management in Transportation Operations. 2009 International Conference;
http://depts.washington.edu/uwconf/fmto/FatigueManagementAbstracts.pdf.
3

Just as the aviation industry, including the NTSB, has addressed alcohol use and adherence to SOPs, it
must also address the issue of fatigue. Unlike many of our complex, technical or cutting edge findings
that require further explanation to the public to show why we made the finding, I believe this situation is
one that requires an explanation of why we did not reach a conclusion – that is, why we did not identify
fatigue in the probable cause determination. Anyone who has attempted to overnight in a crew lounge, an
office or an airport waiting room, or has tried to get a night’s sleep on a red-eye flight from Seattle to
Newark will tell you, this type of sleep in not recuperative, and the data and science support this. Anyone
who has a new baby at home or is caring for an ill relative can tell you that interrupted sleep is not
restorative sleep, and studies support this. Any employee who is asked to remain awake throughout the
day and be prepared for the most demanding portion of their workday at 10pm after they have been awake
for at least 15 consecutive hours would likely acknowledge that they are not at peak performance, and
research supports this. Safety Board studies indicate that the duration of the most recent sleep period, the
amount of sleep during the previous 24 hours, and split or fragmented sleep patterns are among the most
critical factors leading to fatigue-related accidents.
13
The failure of the Safety Board to include fatigue as one of the contributing factors in this accident is
symptomatic of the Board’s inconsistent approach to addressing fatigue in transportation accidents. We
have developed a methodology to be used by our investigators in our on-going efforts to address fatigue
in accident investigations through a fatigue checklist.
14
It is not necessary for fatigue to be the sole cause
of an accident, but it should be included as a factor when it is present and performance deficiencies
consistent with fatigue are identified. In 1999 the NTSB recognized that, “[a]lthough generally accepted
as a factor in transportation accidents, the exact number of accidents due to fatigue is difficult to
determine and likely to be underestimated. The difficulty in determining the incidence of fatigue-related
accidents is due, at least in part, to the difficulty in identifying fatigue as a causal or contributing factor in
accidents. There is no comparable chemical test for identifying the presence of fatigue as there is for
identifying the presence of drugs or alcohol; hence, it is often difficult to conclude unequivocally that
fatigue was a causal or contributing factor in an accident. In most instances, one or more indirect or
circumstantial pieces of evidence are used to make the case that fatigue was a factor in the accidents.”
15
There is consensus at the Safety Board that the flight crew in this accident was likely fatigued, and our
accident report makes this conclusion. The factual information in the docket establishes the presence of
fatigue for both of these crew members.
16
The captain spent the night before the accident sleeping in the
company crew room, where he obtained, at best, 8 hours of interrupted sleep as evidenced by multiple
log-ins to the CrewTrac system at 2151, then 0310 and again at 0726. At worst, it was poor-quality,
interrupted sleep of a shorter duration. NASA and other studies show that even in an onboard rest facility
with beds available for long haul flight crews, pilots might get three hours of sleep and the quality does
not approach 'home' sleep.
17
So, conservatively, the captain in this accident obtained 2 fewer hours sleep
than his usual sleep and perhaps, significantly less based on the quality of sleep. In addition to this acute
13
National Transportation Safety Board, Factors That Affect Fatigue in Heavy Truck Accidents, Highway Safety
Study NTSB/SS-95/01 (Washington, D.C.: NTSB, 1995).
14
http://www.ntsb.gov/info/fatigue_checklist_V%202_0.pdf.
15
SR99-01 - Evaluation of U.S. Department of Transportation Efforts in the 1990s to Address Operator Fatigue
16
National Transportation Safety Board, Aircraft Accident Report: Crash on Approach to Airport Colgan Air, Inc.
Operating as Continental Connection Flight 3407 Bombardier DHC-8-400, N200WQ Clarence Center, New York,
Feb. 12, 2009, Human Performance Group Chairman Factual Report, Docket No. SA-531, and Addendum 1
DCA09MA027.
17
Rosekind, M.R., Gregory, K.B., Miller, D.L., Co, E.L. (2000). Crew factors in flight operations XII: A survey of
sleep quantity and quality in on-board crew rest facilities. (Technical Memorandum 2000-20961). Moffett Field,
CA: NASA and Rosekind, M. R., Gregory, K. B., Miller, D. L., Oyung, R. L., Neri, D. F., & Dinges, D. F. Sleep
quantity and quality of augmented long-haul flight crews in on-board crew rest facilities. Sleep Research, 1997,
26:41.
4

sleep loss, he had a cumulative sleep debt of between 6 and 12 hours, which reflected the 2 to 4 hours of
sleep debt he accumulated over the course of each of the preceding three nights, two of which were spent
in the crew lounge. At the time of the accident, he had been awake at least 15 hours – 3 hours more than
the level at which the 1994 NTSB study identified performance degradation in accident flight crews.
Finally, the accident occurred at the time of day when the captain would normally go to sleep.
The first officer was similarly not properly rested. The night before the accident, she commuted from
Seattle to Newark, changing planes shortly after midnight in Memphis, and arriving in Newark at 0630,
which was 0300 Seattle time. While she may not have experienced cumulative sleep debt, she likely had
some acute sleep loss and, in the preceding 34 hours, had only gotten a maximum of 8.5 total hours of
sleep – 3.5 hours of which were while traveling overnight cross-country (1 ½ hours from Seattle and 2
hours from Memphis to Newark), and the remaining 5 while resting in the company crew room. However,
based on information contained in the docket including an interview of a flight attendant who had a
conversation with the first officer during the 1100 hour, the 5 hours of rest in the crew lounge between
0800 and 1300 are questionable. Again, it is not likely that she obtained recuperative sleep in a busy,
well-lit crew room.
Reflective of these facts, the Safety Board accident report concludes that “[t]he pilots’ performance was
likely impaired because of fatigue…” However, the report diminishes the significance of this finding
when it states that “[sic] the extent of their impairment and the degree to which [fatigue] contributed to
the performance deficiencies that occurred during the flight cannot be conclusively determined.” More
simply, the report concludes that while fatigue likely impaired the pilots’ performance, because we could
not assign fatigue a percent or number, we discount it as a contributing factor of the accident.
This approach is not consistent with our determinations in other accident investigations. For example in
the collision between a truck and an Amtrak train in Bourbonnais,
18
the Safety Board stated that “despite
the fact that the truck driver was suffering from fatigue at the time of the accident, investigators could not
determine the extent to which fatigue accounted for his performance” (analysis page 55). However, that
did not prevent the Board from citing in the probable cause for the accident the truck driver’s
“inappropriate response to the grade crossing warning devices and his judgment, likely impaired by
fatigue.” Similarly, in a collision between two trains in Macdona, Texas,
19
the Safety Board concluded
that “neither the engineer nor the conductor of the Union Pacific Railroad train made effective use of the
time that was available to them to obtain rest.” In that accident, the Safety Board identified fatigue as the
cause of the crew’s inappropriate response to wayside signals governing the movement of their train.
Contributing to the crewmembers’ fatigue was their failure to obtain sufficient restorative rest prior to
reporting for duty because of their ineffective use of off-duty time and the company scheduling practices
which inverted their sleep cycles. In the 1989 grounding of the U.S. tank ship Exxon Valdez, many recall
the intoxication of the ship’s Captain, but this was also a significant fatigue accident. Fatigue was
identified as a major contributor that, subsequently, was given serious national and international attention
when the Board stated that “there were no rested deck officers on the Exxon Valdez available to stand the
navigation watch when the vessel departed from the Alyeska Terminal.”
20
Fatigue was cited in the
probable cause of the accident.
18
National Transportation Safety Board, Collision of National Railroad Passenger Corporation (Amtrak) train 59
with a loaded truck-semitrailer combination at a highway/rail grade crossing in Bourbonnais, Illinois, March 15,
1999.
19
National Transportation Safety Board, Collision of Union Pacific Railroad Train MHOTU-23 With BNSF
Railway Company Train MEAP-TUL-126-D With Subsequent Derailment and Hazardous Materials Release;
Macdona, Texas; June 28, 2004; RAR0603.
20
National Transportation Safety Board, Grounding of U.S. Tank ship Exxon Valdez on Bligh Reef, Prince William
Sound Near Valdez, Alaska, March 04 1989. NTSB/ MAR-90/04, Washington D.C.: NTSB.
5

In other more recent Safety Board aviation accident investigations, the Board concluded that fatigue –
even if unquantifiable – caused or contributed to the accident. For example, in the Shuttle America
accident in Cleveland in 2007
21
, the Board determined that fatigue was one of four contributing factors,
such that the captain’s fatigue affected his ability to effectively plan for and monitor the approach and
landing. Also in 2007, in our investigation of the Pinnacle, Traverse City accident,
22
the Board found that
poor decision making by the pilots likely reflected the effects of fatigue produced by a long, demanding
duty day. In another case, the 2004 Kirksville, Missouri accident,
23
the Board found that the pilots’
fatigue likely contributed to their degraded performance. It is important to note that similar to this
accident, in the CVR transcripts for both the Shuttle America and Kirksville accidents, the crewmembers
are engaged in conversation throughout the flight, chatting about various topics, and in the Kirksville
accident their sterile cockpit violation is also cited in the probable cause. In each of these investigations,
the Safety Board determined that fatigue caused or contributed to the accident. We should be making a
similar determination here.
Presently, we do not have the tools to conclusively determine the degree to which a person is fatigued.
We cannot pinpoint whether fatigue results in 20% memory reduction, 50% degraded decision-making
ability, 25% slower reaction time, or some other value for each individual. This difficulty, however, does
not mean we cannot – or should not – find that fatigue contributed to the accident. Making a
determination that fatigue is a contributing factor does not detract from this accident report’s other
determinations, nor is it an all-or-nothing proposition. A captain can be a poor performer and also be
fatigued. The crew may violate the sterile cockpit rules and be fatigued. A first officer may not adhere to
standard operating procedures and also be fatigued.
The issue of fatigue challenges us to periodically adjust our lens and take a fresh look to ensure that the
aviation industry and the crews who fly our skies report to work rested and fit for duty. Fatigue is
complex and multifaceted. During my time at the Board, we have issued recommendations about sleep
disorders, flight and duty time revisions, fatigue management systems, education and training. I suggest
that our failure to identify fatigue as a factor in this accident is not just a missed opportunity, but also
turns a blind eye to a situation that even the average person can recognize. We are never going to change
the debate on fatigue unless we face it head on. That means dealing with all aspects of fatigue – from
revising the hours of service to sleep disorders to personal responsibility to commuting.
Flight crew commuting is particularly challenging. A regional flight crew’s home base changes often, and
to offset the disruption of frequent relocations, pilots may commute from a home location. The Colgan
Air pilots were commuting pilots. Both pilots were based in ERW but the captain lived in Florida and the
first officer in Seattle. During the previous 14 months, the first officer lived in Phoenix (when hired by the
company), then expected to be based in Houston before being sent to Norfolk, Virginia and then at the
time of the accident, was based in Newark, New Jersey but lived in Seattle, Washington. Flight crew
salaries are also problematic. It is financially challenging for pilots, whether earning $60,000 or $16,000,
to regularly relocate their families or hold down multiple residences. When the FAA convened the fatigue
21
National Transportation Safety Board, Aircraft Accident Report: Runway Overrun During Landing Shuttle
America, Inc. Doing Business as Delta Connection Flight 6448 Embraer ERJ-170, N862RW Cleveland, Ohio
February 18, 2007. AAR-08-01
22
National Transportation Safety Board, Aircraft Accident Report: Runway Overrun During Landing Pinnacle
Airlines Flight 4712 Bombardier/Canadair Regional Jet CL600-2B19, N8905F Traverse City, Michigan April 12,
2007, AAR-08-02.
23
National Transportation Safety Board, Aircraft Accident Report: Collision with Trees and Crash Short of Runway,
Corporate Airlines Flight 5966, British Aerospace BAE-J3201, N875JX, Kirksville, Missouri, October 19, 2004.
AAR-06-01.
6
7
ARC in the summer of 2009, they took commuting off the table, and neither Colgan, nor ALPA addressed
the issue of commuting in their accident submission documents, even though 70% of the pilots based in
Newark commute and 20% commute from over 1000 miles away. I recognize that an objective analysis of
commuting will be a difficult, and perhaps, uncomfortable discussion. But we should not be afraid to
confront this issue in the context of understanding fatigue and its effect on pilot performance.
The one constant throughout this discussion is that the causes of fatigue among pilots are fairly well-
defined and that the results of fatigue, namely accidents of varying degrees, are well-known.
Unfortunately, in the aviation industry, fatigue-related decisions – such as minimum crew hires, flight
crew schedules and commuting – are decisions that too often reflect the economics of the industry, rather
than the data and science of fatigue and human performance.
The tragedy in this accident report is that what we uncovered in the investigation, we already knew.
The FAA talks about safety being their highest priority. Colgan Air’s slogan was never to compromise
safety. The pilots want a safe profession. Yet, if we are serious about safety, we must establish an
aviation system that minimizes pilot fatigue and ensures that flight crews report to work rested and fit for
duty. Flying tired is flying dangerously, and it is a practice that needs to end.

Notation8090C
ConcurringStatementbyVice‐ChairmanChristopherA.Hart
Inconcurringwiththereportandde cisionregardingthis tragicaccident,Icommendthestaffforsucha
thoroughanddetailedinvestigationandreport,andIcommendtheBoardforbringingthebenefitof
variousviewpointsandperspectivestohelpaddresssomeverycomplexanddifficultissues,including
severalissuesonwhichreasonablepeoplecandiffer.Ialsocommendthestaffforrecommendingthat
twoissuesofindustry‐widesignificancebetreatedinanindustry‐widemanner,ratherthansolelyin
relationtothisaccident–(a)pilotprofessionalism,and(b)theimpactuponsafetyofcode‐sharing
arrangementsbetweenmajorandregionalcarriers.Inthisconcurringstatement,Iwouldlikebrieflyto
addressthefirstofthosetwoissuesaswellasFOQA.
PilotProfessionalism
InthesunshinemeetingIstatedmyconcernthatourcommercialaviationsystemisexperiencinga
decliningpercentageofairlinepilotswhohavethebenefitofmilitarypilottraining,andoursystemis
notadequatelyrespondingtothechallengesthatarebeingcreatedbythatdecline.Notonlyismilitary
trainingworld‐class,butthemilitaryhasalonghistoryofeffectivelyweedingoutthosewhosimplylack
“therightstuff.”
Thisisnottosaythatpilotscannotgetworld‐classtraininginourciviliansystem;butthatsystemneeds,
amongotherthings,amoreeffectiveweedingprocess.Currentlythepilotlicensingprocessisbased
uponpassingvariouswrittenandflighttests–butthereisnodistinctionbetweenthosewhopassthe
firsttime,versusthosewhodon’tpassuntilthethirdtime,versusthosewhodon’tpassuntiltheninth
time.Mostofwhatmostattorneysdoisnotpotentiallylife‐threateningfortheirclients,yetsome
stateslimitthenumberoftimesthatlawyers‐to‐becanfailthebarexam. Inaddition,Iamawareofat
leastonemodeoftransportationinwhichfailuretopassacriticalwrittentestthesecondtimeresultsin
dismissalfromtheprogram,andpassingthetestrequiresascoreof100.
Similarly,thereisnodistinctioninourciviliansystembetweenthosewhopassf lightteststhefirsttime
versusthose,suchasthecaptaininthisaccident,whofailedthefirstattemptinseveraldifferentflight
tests.
Moreover,writtentestslargelymeasureknowledge,andflighttestslargelymeasure“stickandrudder”
skills.”Othercrucialattributesarenotgenerallymeasuredbyeitherofthesetests,suchasdiscipline

2
andjudgment–twoattributesforwhichtheeffectivenessofmilitarytrainingisalsowellknown,but
thathavealsobeenshownlackinginthisandotherrecentcommercialaviationaccidentsandincidents.
Ourciviliansystemneedstoaddressthechallengeofsystematicallycontinuingtoprovidetheworld‐
classpilottrainingthatthemilitaryhasprovidedforsomanyyears,andthesystemparticularlyneedsa
betterwaytokeepoutthosewhoshouldnotbeginorcontinueflyingpassengersforhire.
FlightOperationalQualityAssurance(FOQA)
BeforecomingtotheNTSBIwasinvolvedindevelopi ngandfacilitatingvariousproactiveinformation
programsattheFAA,andindoingso,IhavefrequentlystatedmyoppositiontomandatingFOQA
programs.VoluntaryFOQAprogramsintheUSprovidedmuchofthecrucialinformationthatthe
industrysafetyprocessesusedtodecreasetheUSfatalaccidentrateby65%fro m1997to2007–
amazingenoughinandofitself,butevenmoresogiventhattheindustrywasalreadygenerally
consideredtobeverysafein1997.MandatingFOQAinthewakeofthatsuccessstorycouldbeviewed
as“punishing”thosewhodidtherightthing,andrunstheriskofmakingtheperfect,i.e.,100%
implementationofFOQA,theenemyofthegood.
InaworldinwhichFOQAprogramsarenotaswidelyimplementedastheyareintheUS,Icertainly
understandwhyICAOwantsthemmandated;butintheUS,wherevoluntaryimplementationisso
widespread–thevastmajorityofpassengersintheUSarecarriedonairlineswithFOQAprograms–the
needforamandateisnotsoapparent.
OneofmymajorconcernsaboutmandatingFOQAisthatamandatecouldresultinalossofthe
protectionthatFOQAinformationcurrentlyhaswhenitissharedwiththeFAA.Whentheproposalwas
offerednottorequiresharingoftheinformationwiththeFAAunlessanduntillegislationisobtained
thatprotectsinformationthatissharedwiththeFAA,Ifeltthatitwouldbebetterforthesafetyofthe
systemtoconcurwithamandaterecommendation,assomodified,ratherthanhavingthemandate
recommendationbeadoptedbymajorityvote,overmydissent,asitwasoriginallyproposed.

NTSB Aircraft Accident Report
5. Appendixes
Appendix A
Investigation and Hearing
Investigation
The National Transportation Safety Board was notified of this accident about 2230 on
February 12, 2009. A go-team launched early the next morning. Accompanying the team to
Buffalo was former Board Member Steven Chealander.
The following investigative teams were formed: Operations, Human Performance,
Structures, Systems, Powerplants, Air Traffic Control, Meteorology, Aircraft Performance,
Maintenance Records, and Pipeline. Also, specialists were assigned to conduct the readout of the
flight data recorder and transcribe the cockpit voice recorder at the NTSB’s laboratory in
Washington, D.C.
Parties to the investigation were the Federal Aviation Administration (FAA), Colgan Air,
Air Line Pilots Association (ALPA), National Air Traffic Controllers Association, and United
Steelworkers Union (Flight Attendants). In accordance with the provisions of Annex 13 to the
Convention on International Civil Aviation, the Transportation Safety Board of Canada (TSB)
participated in the investigation as the representative of the State of Design and Manufacture
(Airframe and Engines), and the Air Accidents Investigation Branch of the United Kingdom
(AAIB) participated in the investigation as the representative of the State of Design and
Manufacture (Propellers). Transport Canada, Bombardier, and Pratt & Whitney Canada
participated in the investigation as technical advisors to the TSB, and Dowty Propellers
participated in the investigation as a technical advisor to the AAIB, as provided in Annex 13.
Public Hearing
A public hearing was held from May 12 to 14, 2009, in Washington, D.C. Former Acting
Chairman Mark Rosenker presided over the hearing; Board Member and current Chairman
Deborah Hersman, former Board Member Kathryn Higgins, and Board Member Robert Sumwalt
also participated in the hearing. The issues presented at the hearing were the effect of icing on
airplane performance, cold weather operations, sterile cockpit rules, flight crew experience,
fatigue management, and stall recovery training.
The technical panel comprised investigators from the NTSB and the TSB. Parties to the
public hearing were the FAA, Colgan Air, ALPA, and Bombardier.
174
NTSB Aircraft Accident Report
175
Appendix B
Cockpit Voice Recorder
The following is a transcript of the Honeywell model 6022 SSCVR 120 cockpit voice
recorder, serial number 97896, installed on a Bombardier DHC-8-400, N200WQ, operated by
Colgan Air, Inc., as Continental Connection flight 3407, which crashed into a residence in
Clarence Center, New York, while on an instrument approach to Buffalo-Niagara International
Airport, Buffalo, New York, on February 12, 2009:
LEGEND
CAM Cockpit area microphone voice or sound source
HOT Flight crew audio panel voice or sound source
INT Interphone voice or sound source
PA Public address sound source
RDO Radio transmissions from N200WQ
RAMP Radio transmission from Newark Ramp controller
GND Radio transmission from Newark Ground controller
TWR Radio transmission from the Newark Tower controller
DEP Radio transmission from New York Departure controller
ZNY Radio transmission from the New York Center controller
ZOB Radio transmission from the Cleveland Center controller
APP Radio transmission from the Buffalo Approach controller
OPS Radio transmission from the Colgan Buffalo Operations ground controller
-A First controller at identified ATC facility
-B Second controller at identified ATC facility
-C Third controller at identified ATC facility
-1 Voice identified as the captain
-2 Voice identified as the first officer
-3 Voice identified as the flight attendant
-? Voice unidentified
* Unintelligible word
# Expletive
@ Non-pertinent word
( ) Questionable insertion
[ ] Editorial insertion
Note 1: Times are expressed in Eastern Standard Time.
Note 2: Generally, only radio transmissions to and from the accident aircraft were transcribed.
Note 3: Words shown with excess vowels, letters, or drawn out syllables are a phonetic representation of the words
as spoken.
Note 4: A non-pertinent word, where noted, refers to a word not directly related to the operation, control or condition
of the aircraft.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
176
20:15:48
START OF RECORDING
START OF TRANSCRIPT
20:16:03.4
HOT-1
heard somebody on the— on the phone earlier today before I saw you for
the first time this morning. I believe it was— yeah yeah it was before that.
that uh was talking about you know possibly getting Qs later this year.
20:16:11.0
HOT-2
uh-huh… oh yeah?
20:16:23.3
HOT-1
so there's been some scuttlebutt...uh...
20:17:30.3
RAMP
Colgan thirty four oh seven monitor ground on point eight. he'll be
with you in about uh five minutes.
20:17:35.7
RDO-2
over to ground Colgan thirty four zero seven.
20:17:43.2
HOT-2
yeah I've heard so many things and people say this and people say that.
20:17:47.3
HOT-1
yeah.
20:17:47.6
HOT-2
I'm just— I'm surprised at how calmly— I usually don't do very well with
not knowing what's happening. I like to know exactly what it's going to be
you know in my future for the next day the next week the next month. and
I'm just— now that I'm commuting from Seattle I'm thinking you know it
really doesn't matter where you know I would— if it went anywhere else
I'd put in a bid to go anywhere but Newark. I can't get farther away from
Seattle really...well so much I like Florida but I just have never heard any
of those rumors.
20:18:20.8
HOT-1
no I haven't either.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
177
20:18:22.1
HOT-2
or Atlanta.
20:18:22.8
HOT-1
actually the the the Saab would do pretty well as long as they weren't on
uh they would never go on derivative power. [sound of throat clearing]
they have a derivative uh— oh man DC ten. or an MD eleven. one of the
two.
20:18:36.2
HOT-2
**.
20:18:41.3
HOT-1
FedEx. oh you know those guys. that was like a carrier landing to them.
20:18:45.2
HOT-2
yeah.
20:18:49.1
HOT-1
um anyway uhhh— what was I gonna say...oh the Saab.
20:18:57.1
HOT-2
yeah.
20:18:57.3
HOT-1
they have a derivative engine program that uhh you know when the
engine starts producing less then then rated power you know they— then
we go into a derivative situation. the only time it hurts which would really
hurt in Florida obviously is when it's hot and heavy.
20:19:05.7
HOT-2
uh-huh...yeah.
20:19:16.8
HOT-1
you know it doesn't climb for beans. but but as far as— I flew the nineteen
hundred in in Florida and to go down there in the summertime in the
afternoon when the thunderstorms are all developing and everything that
nineteen hundred gets tossed around pretty good.
20:19:35.5
HOT-2
yeah.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
178
20:19:36.1
HOT-1
but the uh the three forty is pretty solid. it it uh it bounces around but it it's
so much heavier than the nineteen hundred it doesn't— it doesn't do too
bad.
20:19:47.3
HOT-2
yeah I was flying in Flagstaff and the density in Arizona— the density
altitude of I think it's like eleven thousand five hundred.
20:19:56.8
HOT-1
uh-huh.
20:19:58.5
HOT-2
and that I was just in like an Arrow— a Piper Arrow. but the runway
slopes a little bit and you can't climb faster than the runway slopes like
you'll take off and then the runway slopes up a little bit— Sedona does the
same thing and I was there around the same week when it was just
horrible density altitude. and you'd take off and my students would try to
pull the nose up and I'd push it right back down and you know you'd hit
the runway again before you can get enough speed to actually get up and
off the ground. it's really not a very comfortable feeling.
20:20:24.5
HOT-1
wow.
20:20:27.5
HOT-2
but when it's a hundred and twenty down in Phoenix and you get a little bit
higher in the mountains and you know it's still it's cooled down to a
hundred and five but you're at you know seven thousand feet altitude.
20:21:22.9
HOT-2
I was in one of those this morning.
20:21:25.4
HOT-1
yeah.
20:21:26.1
HOT-2
I was in one of those this time last night.
20:21:41.2
HOT-1
ohhh heavens.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
179
20:22:23.7
HOT-1
you know the bad thing is is uh because they you know cancelled the
Rochester round trip— or wherever we were going— was it Rochester?
yeah I think it was.
20:22:33.7
HOT-2
yeah. now this doesn't mean anything.
20:22:35.7
HOT-1
this doesn't mean anything. you know you can't uh make a dime off of
this.
20:22:41.0
HOT-2
yeah although I'm still excited about flight time so. [sound of laughter] I'm
glad you know the more flight time I get the better.
20:23:14.1
HOT-?
[sound of sniffle]
20:23:14.5
HOT-2
no and they— I told you that they dropped a four day trip from my PC
check.
20:23:18.8
HOT-1
yeah yeah yeah.
20:23:19.4
HOT-2
yeah so I think I'm at like sixty five hours or so anyways. it it would take a
lot of over to get me up there.
20:23:33.1
HOT-2
did you see the lines for next month?
20:23:35.3
HOT-1
shew. yeah I saw them. not good for me. [sound of throat clearing]
20:23:39.4
HOT-2
ohhh. I printed them out I didn't look at them.
20:23:43.2
HOT-1
I'll be in the back. just a sec.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
180
20:23:44.7
HOT-2
I got one.
20:23:46.7
PA-1
folks from the flight deck just to keep you updated. uh we're we're gonna
be sitting here just for a few more minutes uh... we did have some taxi
delays out there obviously because of the uh the weather. uh planes are
moving right now we're about number twenty uh for takeoff so it'll be uh
it'll probably be another forty minutes. forty to forty five minutes before
we're airborne. I appreciate your patience.
20:24:15.2
HOT-1
[sound of throat clearing]
20:24:30.3
HOT
[sound of double chime]
20:24:34.9
INT-1
what's up?
20:24:35.3
INT-2
hi. passengers would like to know if they can use cell phones. they all
need to do some calls.
20:24:39.5
INT-1
oh I I figured as much. I thought about that right whenever uh I got done.
20:24:46.1
INT-3
that be okay?
20:24:46.7
INT-1
and I was just waiting for the call. I knew you were gonna call. I was just
you know I was surprised you didn't call fifteen seconds earlier.
20:24:49.1
INT-3
[sound of laughter]
20:24:55.2
INT-3
and were gonna go ahead and give ‘em some water. is that okay?
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
181
20:24:58.2
INT-1
uh yeah but be careful because I may be moving up here just you know in
just a little while just to a different place.
20:25:03.8
INT-3
okay. okay that's fine.
20:25:05.3
INT-1
and if you guys want to be up and uh do some water or something that'll
be good.
20:25:07.2
INT-3
yeah yeah just in case we can't do any service in the air. ‘cause I have to
tell you a lot of them are not very happy so we'll try to get them happy.
[sound of laughter]
20:25:15.7
INT-1
okay that sounds wonderful. okay thanks.
20:25:16.8
INT-3
thanks. alright.
20:25:30.0
PA-3
ladies and gentlemen if you need to use your cellphones I have asked the
captain and he said that it would be okay. thank you.
20:25:39.5
HOT-?
[sound of sniffle]
20:25:49.1
HOT-1
ohh heavens...I am glad I came over to the uh Q. my— my whole deal
with uh you know comin' over even though I'm kind of getting screwed on
the on the schedules.
20:26:05.6
HOT-2
yeah.
20:26:06.0
HOT-1
and I'll you how uh what it will do is if these things go to Houston in six
months or nine months or whatever I'm already in the Q.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
182
20:26:16.5
HOT-2
yeah.
20:26:19.3
HOT-1
uh there are a lot of guys in Houston right now that have more seniority
than I do uh um that refuse to go to the Q until it gets to Houston.
20:26:31.3
HOT-2
yeah.
20:26:32.1
HOT-1
so I figured well you know I'll go ahead and jump in the Q.
20:26:36.5
HOT-2
yeah.
20:26:37.0
HOT-1
uh maybe I'll be able to uh take another day off.
20:26:39.7
HOT
[sound of double chime]
20:26:41.2
HOT-1
I'll get it.
20:26:43.1
INT-1
yes?
20:26:43.5
INT-3
what about using the lav? we've got a couple of people that are a little
annoyed because we're telling them they can't use the lav.
20:26:51.3
INT-1
uh well you know as long as I'm sittin' here uh let me know whenever
they're seated because I I don't know when they're gonna— when they're
gonna release us to uh to move. uh but go ahead and just keep us
updated for each and every person that gets up to go to the lav I need to
know when they're seated. when they're seated.
20:27:09.1
INT-3
oh okay.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
183
20:27:09.7
HOT-1
okay?
20:27:10.4
INT-3
alright.
20:27:11.1
INT-1
alright.
20:27:11.5
INT-3
alright.
20:27:11.8
INT-1
tell them to piss off early.
20:27:14.9
HOT-2
[sound of laughter]
20:27:17.7
HOT-2
[sound of throat clearing]
20:27:30.8
HOT-1
anyway. um you know I jumped on this thing. I figured you know I was
busting my butt on the on the Saab.
20:27:39.2
HOT-2
yeah.
20:27:39.8
HOT-1
um my philosophy is it's all about the pay credit.
20:27:44.3
HOT-2
uh-huh.
20:27:44.6
HOT-1
'kay that's what I live and breath by but uh I mean I had one month last
summer uh July or August. had a hundred forty seven hours of pay credit.
20:27:59.0
HOT-2
yeah...that's nice.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
184
20:27:59.4
HOT-1
that was sweet. and and I you know I never did but I thought man if I— if I
was on the Q—.
20:28:05.5
HOT
[sound of double chime]
20:28:07.3
HOT-2
that'd be so much more.
20:28:08.3
HOT-1
yeah oh gosh yeah.
20:28:09.2
INT-2
howdy.
20:28:10.3
INT-3
I have someone in the lav right now and then there'll be another person
going in and I'll let you know when they're out and seated. okay?
20:28:17.1
INT-1
alright.
20:28:17.5
INT-3
alright thanks.
20:28:19.9
HOT-1
um but you know once I get down there it's gonna take a month month
and a half for everybody to go through you know how ever many they
take at a time.
20:28:27.9
HOT-2
yeah.
20:28:30.4
HOT-1
once it gets down there. plus there's also a bunch of other guys that are
here that uh—.
20:28:36.6
HOT-2
[sound of sneeze]
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
185
20:28:37.4
HOT-1
bless you. that want to uh go back to Houston.
20:28:41.9
HOT-2
yeah.
20:28:42.9
HOT-1
a bunch.
20:28:45.4
HOT-2
there's a ton of em.
20:28:48.8
HOT-1
there's uh there's even a few that uh have never been to Houston [sound
of laughter] that want to get the heck out of Newark.
20:28:54.5
HOT-2
that's that's me.
20:28:55.8
HOT-1
so—.
20:28:56.8
HOT-2
I'll go. I'll put in a bid for wherever this thing goes. I figured they— if it went
to Houston there might be some more FOs that would want to transition
over but they'd let me go down before they transition other guys over
wouldn't they? yeah.
20:29:08.1
HOT-1
oh sure oh sure. because they would let you go as the openings are
available and your seniority dictates.
20:29:14.4
HOT-2
yeah yeah.
20:29:16.3
HOT-1
uh once you get down there and and this would be very similar to me.
20:29:20.8
HOT-2
yeah.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
186
20:29:21.1
HOT-1
uh—.
20:29:22.7
HOT-2
they can't kick me out once they allowed me down there though can they?
20:29:25.1
HOT-1
oh no no.
20:29:25.9
HOT-2
yeah.
20:29:26.6
HOT-1
but it but it would happen the exact same thing with me as it would with
you.
20:29:31.8
HOT-2
yeah.
20:29:32.4
HOT-1
we get down there shew we get this schedule this schedule this schedule
and as they kept as they keep transitioning people over our schedules get
worse and worse and worse.
20:29:36.3
HOT-2
yeah yeah worse and worse and worse.
20:29:43.8
HOT-1
but uh you know that's that's in the future we'll see what happens.
20:29:44.5
HOT-2
[sound of sniffle]
20:29:49.0
HOT-2
yeah.
20:29:50.0
HOT-1
but even on the Saab uh I was able to make about uh gross about sixty
thousand last year so—.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
187
20:30:02.4
HOT-2
I made gross fifteen thousand eight hundred. I got here in January. aww.
20:30:03.0
HOT-1
but I— yeah no I know no I know. I I understand. I was on the on the uh
FO uh welfare—.
20:30:12.9
HOT-2
you were there when it was nineteen an hour weren't you?
20:30:15.4
HOT-1
no I never was on nineteen. no.
20:30:16.3
HOT-2
[sound of sniffle] oh. that's good.
20:30:20.1
HOT-2
I'm just lucky 'cause I have a husband that's working.
20:30:22.2
GND
Colgan thirty four zero seven you're at romeo mike correct?
20:30:25.4
RDO-2
uh romeo hotel Colgan thirty four zero seven.
20:30:27.6
GND
okay Colgan thirty four zero seven out of romeo hotel roger. you're
gonna give way to Delta from the left and then taxi via bravo and
hold short of kilo.
20:30:37.8
RDO-2
give way to Delta then bravo short of kilo for Colgan thirty four zero
seven.
20:30:41.8
HOT-2
[sound of sniffles]
20:30:42.8
HOT-1
alright give way to Delta then I'm sorry.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
188
20:30:44.5
HOT-2
bravo short of kilo.
20:30:45.6
HOT-1
bravo short of kilo.
20:30:46.8
HOT-2
I don't see a Delta.
20:30:48.0
HOT-1
right here. this uh plane here.
20:30:50.0
HOT-2
oh gotcha.
20:30:51.9
HOT
[sound of double chime]
20:30:55.6
HOT-1
[sound of throat clearing]
20:30:56.8
INT-3
hello?
20:30:57.9
INT-1
hey are they are they back?
20:30:58.6
INT-3
I still have another one in the bathroom and another one waiting. do you
need—.
20:31:02.6
INT-1
no I uh I uh we need to go.
20:31:04.9
INT-3
okay uh.
20:31:05.1
INT-1
so the one waiting has to wait and I I'm gonna have to coordinate to uh.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
189
20:31:05.8
INT-3
okay okay. one in there right now as soon as she comes out I'll—.
20:31:14.7
INT-1
alright well this is— I was afraid of this. alright thanks.
20:31:16.3
INT-3
okay okay alright.
20:31:25.5
HOT-2
she might get out in time.
20:31:30.0
HOT-1
God.
20:31:34.4
CAM
[sound similar to door closing]
20:31:35.4
HOT-2
there you can hear her getting out now.
20:31:36.8
HOT-1
yeah.
20:31:42.4
HOT-2
totally lose our spot you can hear him.
20:31:49.3
HOT-2
here I go.
20:31:49.7
HOT
[sound of double chime]
20:31:50.4
INT-2
that it?
20:31:51.3
INT-3
okay we're good.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
190
20:31:55.6
HOT-?
[sound of sniffle]
20:32:15.2
HOT-1
I hate to make people wait. I understand needs and all that kind of stuff
but uh.
20:32:17.4
HOT-2
oh I know but if it means us taking off and us three people later in line.
20:32:48.3
HOT-1
alright bravo short of kilo.
20:33:05.6
HOT-1
yeah we're on ground now right?
20:33:08.8
HOT-2
yeah.
20:33:10.0
HOT-?
[sound of sniffle]
20:34:02.1
HOT-?
[sound of sniffle]
20:34:06.5
GND
Colgan thirty four zero seven Newark Ground two two right at
whiskey continue juliet at romeo follow JetBlue.
20:34:14.4
RDO-2
juliet at romeo follow JetBlue Colgan thirty four zero seven.
20:34:18.5
HOT-1
yeah JetBlue's right behind uh the bent wing pencil jet.
20:34:25.7
HOT-2
[sound of laughter]
20:34:27.0
HOT-1
looked like a bent wing maybe it's not.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
191
20:34:31.2
HOT-2
what's that mean?
20:34:31.8
HOT-1
it's just a lawn dart.
20:34:33.0
HOT-2
oh I've never heard the term bent wing.
20:34:37.3
HOT-1
bent wing is winglet.
20:34:39.1
HOT-2
oh oh gotcha.
20:35:16.7
HOT-2
come on JetBlue. I didn't realize JetBlue came in to here. I wonder where
they go from.
20:35:22.7
HOT-1
they have uh one flight to Tampa they have uh couple flights to Fort
Lauderdale and uh three or four flights to Orlando.
20:35:30.7
HOT-2
out of Newark?
20:35:31.9
HOT-1
out of Newark.
20:35:33.6
HOT-2
oh okay well that doesn't help me at all. 'cause JetBlue does a ton—
there's like four flights from Seattle to JFK a day and I decided I figured it
out that'd be you know if I'm only doing it a couple times a week or a
couple times a month or like once a month. that's only— I think there's a
twenty five dollar shuttle.
20:35:51.1
HOT-1
yeah.
20:35:52.1
HOT-2
that's not so bad.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
192
20:35:53.9
HOT-1
they have free TV. live TV.
20:35:55.7
HOT-2
on the shuttle?
20:35:57.1
HOT-1
on uh JetBlue.
20:35:57.7
HOT-2
oh on JetBlue.
20:35:58.8
HOT-1
you got to pay for your for your movies though. if you ever— if you fly
Continental if they fly seven fives or the uh seven three nine hundreds the
ones that are equipped you got free movies.
20:36:13.2
HOT-2
that's cool.
20:36:13.4
GND
Lufthansa four one three heavy at juliet follow the Continental
Express Embraer— make that the Continental uh Dash eight Q four
hundred series.
20:36:19.6
HOT-2
Q four hundred.
20:36:33.0
GND
Colgan thirty four zero seven you follow JetBlue that's your
sequence about number sixteen. monitor the tower.
20:36:39.8
RDO-2
follow JetBlue and monitor tower Colgan thirty four zero seven.
20:36:48.2
HOT-?
[sound of sniffles]
20:37:11.4
PA-3
ladies and gentlemen at this time once again if you'd be so kind and turn
off your cell phones. thank you.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
193
20:37:17.8
HOT-2
you think they'd just be launching us off two two since all these planes
have circle to land two nine...you'd think they'd be using the right and the
left. [sound of sniffle] well I guess never mind because then you've got
spacing going to the—.
20:37:35.5
HOT-1
yeah the spacing off the arrivals still because uh until they break.
20:37:37.4
HOT-2
yeah. that's right I forget about all that.
20:37:59.9
HOT
[sound of master caution chime]
20:38:00.7
HOT-?
[sound of sniffle]
20:38:03.4
HOT
[sound of double chime]
20:38:05.4
INT-3
hello?
20:38:06.1
INT-1
hey if that one would like to go to the restroom now go ahead.
20:38:09.1
INT-3
oh okay thank you.
20:38:10.6
INT-1
and let me know if anybody else is in need uh after that one.
20:38:14.1
INT-3
okay thank you. buh-bye.
20:38:14.7
INT-1
okay thanks.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
194
20:38:19.3
HOT-1
oh let's see. what was I gonna tell— I was gonna tell you something. I
didn't want to really say it off of uh in front of the ramp guys.
20:38:28.1
HOT-2
oh you didn't have your FOPP. [Flight Operations Policies and
Procedures Manual]
20:38:29.6
HOT-1
oh yeah yeah yeah yeah yeah yeah uh you know @ right?
20:38:34.3
HOT-2
yeah.
20:38:34.9
HOT-1
um he was doing his PC check today.
20:38:37.4
HOT-2
uh-huh.
20:38:38.0
HOT-1
he came up last night and he's you know he's always been real good you
know as far as just uh seems like a top notch guy.
20:38:45.9
HOT-2
yeah.
20:38:46.3
HOT-1
and he came in and he just— uh it just looked like his face was drained
you know all the blood out of it and everything. he just came in told me he
was headed to his PC check today. and he said he got on the plane he
went to pull it out to uh to study.
20:39:05.5
HOT-2
he was using it to study yeah.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
195
20:39:07.6
HOT-1
and he said it was not in his bag. says that was the first time he uh uh he
figured out that he didn't have it. he left it at home. he says I've been with
the company I forget what he said five or six years this is— this is the first
time he's ever done that. I said dude it happens to the best of us. I said
let's see if we can help you out so I gave him mine I said yeah I just got to
make sure my FO has it you know tomorrow. we ha— we have to have
one in the—.
20:39:36.8
HOT-2
yeah I've got mine.
20:39:37.9
HOT-1
and so that's all we have to have. but uh made sure it was up to date um
which it was and uh he took it down there.
20:39:51.1
HOT-2
that was nice of you.
20:39:52.9
HOT-1
and he was he was coming in from Saint Lou— uh coming in from Saint
Louis. he was gonna try to and make the one thirty flight today to get in at
five oh clock.
20:40:03.0
HOT-2
to Saint Louis?
20:40:04.3
HOT-1
in. one thirty out of Saint Louis in here at five oh clock.
20:40:07.8
HOT-2
oh yeah?
20:40:08.3
HOT-1
and that flight was delayed until five thirty so he wasn't going to be in until
uh about— what time is it now? eight oh clock it's eight forty yeah it's uh
it's due in about any time.
20:40:20.0
HOT-2
yeah...yeah.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
196
20:41:31.1
HOT-?
[sound of sniffle]
20:41:34.5
HOT-2
oh I'm ready to be in the hotel room.
20:41:38.2
HOT-1
I feel feel feel bad for you as far as feeling **.
20:41:44.2
HOT-2
well this is one of those times that if I felt like this when I was at home
there's no way I would have come all the way out here. but now that I'm
out here.
20:41:51.7
HOT-1
you might as well.
20:41:52.7
HOT-2
I mean if I call in sick now I've got to put myself in a hotel until I feel better.
you know we'll see how how it feels flying. if the pressure's just too much I
you know I could always call in tomorrow at least I'm in a hotel on the
company's buck but we'll see. I'm pretty tough.
20:42:09.3
HOT-?
[sound of sniffle]
20:42:15.3
HOT-1
oh that Airborne may help out a little bit.
20:42:18.4
HOT-2
yeah.
20:42:19.1
HOT-1
you could kill it with uh you know a bunch of OJ or a bunch of vitamin C.
20:42:24.1
HOT-2
yeah I've got um got ‘em to give me a a carton of orange juice to take
home with me.
20:42:51.6
HOT-1
is that a triple seven? for TAP? oh nope it's an Airbus three thirty.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
197
20:42:55.7
HOT-2
no it's an Airbus.
20:43:00.8
HOT-?
[sound of sniffle]
20:43:10.2
HOT-2
so what did you do before you started flying for Colgan?
20:43:13.6
HOT-1
oh I I'd been in the airline industry for a while. I worked for uh the original
Piedmont Airlines merged with US Airways. watched two companies—
two profitable companies with two completely different cultures uh merge
together and turn to a pile of crap.
20:43:33.5
HOT-2
oh that's too bad.
20:43:34.8
HOT-1
and I lost my job in the— in the merger.
20:43:39.0
HOT-2
how'd you lose your job?
20:43:40.5
HOT-1
uh they took the position that I was doing— um do you have any napkins
over there by chance?
20:43:45.6
HOT-2
oh yeah I've got a whole load of them in my thing.
20:43:48.6
HOT-1
[sound of coughing]
20:43:50.2
HOT-1
thanks. uh they made my— well I I I guess I could— don't mean to say I
lost my job but uh they gave me a a very poor choice to make.
20:44:03.3
HOT-2
yeah.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
198
20:44:03.8
HOT-1
or a very poor alternative.
20:44:06.6
HOT-2
what was that?
20:44:07.1
HOT-1
uh I was in a management position— well I was temporarily in a
management position. and because I was temporarily in that
management position for longer than thirty days they considered me part
of that department although I was not being paid the full management
salary I was just getting a little uh...
20:44:10.2
HOT-2
[sound of sniffle] uh-huh...yeah.
20:44:33.1
HOT-1
...whatever you want to call it. uh a little add on. and anyway so uh they
turned that position into a clerical position.
20:44:37.1
HOT-2
[sound of sniffle]
20:44:49.7
HOT
[sound of double chime]
20:44:54.4
INT-3
yes sir.
20:44:54.9
INT-1
hey is everyone down?
20:44:56.4
INT-3
yeah.
20:44:57.3
INT-1
okay thanks.
20:44:57.9
INT-3
okay.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
199
20:44:59.7
HOT-1
um so they gave us uh an alternative uh an option to stay with the job it
was going to a clerical position. we would lose approximately sixty five
percent of our salary.
20:45:14.6
HOT-2
whoa.
20:45:15.8
HOT-1
um or you know sayonara so I went sayonara.
20:45:23.9
HOT-2
yeah I would too.
20:45:26.6
HOT-1
and then I worked for American Express for a while as a contract— a
contract employee with RJ Reynolds tobacco company.
20:45:36.0
HOT-2
oh yeah.
20:45:36.6
HOT-1
and uh did a lot of travel packages hospitality events driver appearances
20:45:42.6
HOT-2
oh that's cool.
20:45:43.5
HOT-1
uh for uh for NASCAR uh NHRA track racing AMA superbikes unlimited
hydroplane. that was— that was probably the best job I've ever had.
probably the best one ever. just the most fun. it was challenging at times
yet it was very rewarding you get to go to to the events and all that kind of
stuff.
20:46:04.0
HOT-2
oh I bet. why'd you leave there?
20:46:07.8
HOT-1
uh the uh political uh arena with uh the tobacco companies and smoking
in in general and that stuff.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
200
20:46:14.8
HOT-2
oh.
20:46:18.4
HOT-1
uh the biggest thing that I ever learned in a business law class is uh US
domestic laws are dictated by social acceptance. had a textbook about
this thick.
20:46:28.7
HOT-2
yeah.
20:46:29.4
HOT-1
that was one sentence out of the— one of the chapters.
20:46:33.3
HOT-2
uh-huh.
20:46:33.6
HOT-1
that has stuck with me ever ever since I took that business law class.
20:46:37.7
HOT-2
oh that's funny.
20:46:38.4
HOT-1
and it is so true.
20:46:39.7
HOT-2
yeah.
20:46:40.3
HOT-1
uh I mean there's just so many examples that you could use. and and and
look back and say that's true as true could be. but uh so they were cut
back— oh and I did the sweepstakes stuff too. uh that was a whole
messload of fun.
20:46:58.8
HOT-2
oh yeah?
20:46:59.0
HOT-1
they'd have different sweepstakes for their different uh cigarette brands.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
201
20:47:01.8
HOT-2
uh-huh.
20:47:02.0
HOT-1
and like they'd have the uh uh Salem cigarettes their menthol brand. uh
Salem's fortieth anniversary when the did uh they did forty winners for a
three night cruise in the Bahamas.
20:47:20.0
HOT-2
oh that's cool.
20:47:21.0
HOT-1
so uh they gave me— basically they— uh I develop a package uh wrote
all the little fine print went through legal with that made sure I was okay
and uh then I just waited. waited until they had the drawing and they gave
me a list of forty names. it wasn't just myself uh I was— I was the main
contact point but uh I had two other people that uh helped me out with
that and we had a whole a blast of fun. I mean we'd contact the winners
and say you know this is so and so from American Express Travel on
behalf of RJ Reynolds Tobacco Company and uh we have your name and
we'll do your travel. uh and this is what's planned. this is you know all
kinds of things to do. so anyway I did that as well.
20:47:26.9
HOT-2
yeah...yeah.
20:48:12.7
HOT-1
but uh just with all the political mumbo jumbo they uh they were cutting
back on their brand promotions and sweepstakes and everything.
20:48:20.5
HOT-2
yeah.
20:48:20.8
HOT-1
so uh uh I transferred with American Express and went down— back
down to Tampa er back down to Florida. I was in Orlando to get my **. but
uh after that I worked for Verizon for a little while.
20:48:28.4
HOT-2
yeah....Horizon?
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
202
20:48:39.5
HOT-1
Verizon.
20:48:41.1
HOT-2
oh Verizon. oh okay.
20:48:41.2
HOT-1
Veri— yeah. uh worked in the uh high speed internet uh division.
20:48:45.6
HOT-2
okay.
20:48:46.3
HOT-1
uh sold DSL and all the peripherals that go along with it. DSL and dial up
and helped uh I was on the beta team for uh uh their FTTP is what we call
just the FTTP FTTP program which is fiber tooth the premise is now
called Verizon FIOS.
20:49:06.6
HOT-2
yeah okay.
20:49:10.0
HOT-1
and FIOS is out in uh would be out in the Seattle areas— some of the
Seattle areas uh—.
20:49:17.1
HOT-2
they just did that in the apartments that I was at in the Chesapeake I
think.
20:49:20.7
HOT-1
yeah yeah they go in and do uh you know like uh like an exclusive
arrangement with a— with a community whether it's a you know a
housing community a development or something like that or a condo
community or you know apartments or whatever. they'll go in and do like
an exclusive arrangement for x number of years and then go in and sell it
to everybody give them a good price. but uh we developed all the the
policies and procedures the setup. all that kind of stuff.
20:49:21.8
HOT-2
yeah.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
203
20:49:26.7
HOT
[sound of master caution chime consistent with parking brake application]
20:49:56.3
HOT-2
oh that's neat.
20:50:01.1
HOT-1
so that was neat. they— they gave they gave a big package to
management employees. it was geared toward the old uh technology
people in management positions. uh but they extended it— extended it to
everybody except wireless. and I wasn't in you know I wasn't part of
wireless so I I took the package and left and went flying.
20:50:32.7
HOT-2
okay.
20:50:32.9
HOT-1
I went through Gulfstream's program 'cause uh you know it was just the
best program for for my needs and and what I needed you know the
timeframe that I had. you know how fast I wanted to get into the one
twenty one environment and all that. so it really uh really worked out well
for me.
20:50:56.9
HOT-2
that's good.
20:50:58.3
HOT-1
got hired with Colgan right after that.
20:51:01.5
HOT-2
you've been here you said four years?
20:51:03.4
HOT-1
what's that?
20:51:04.7
HOT-2
you said you've been here four years?
20:51:06.1
HOT-1
uh almost four years. about eh three and a half years.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
204
20:51:17.9
HOT-1
silly old Gulfstream they uh— I even had an interview with Pinnacle to go
fly uh the RJs because they had a preferential program with uh
Gulfstream preferential— preferential interview process.
20:51:29.3
HOT-2
oh yeah?
20:51:32.1
HOT-1
and uh I turned down the job because at that time they weren't they
weren't paying anything for training.
20:51:40.6
HOT-2
oh yeah?
20:51:46.6
HOT-1
they just at that at that point in time I just like well if the company can't
even invest in their employees as they go through training you know
some sort of uh stipend or or something like that. fifty dollar a day per
diem or—.
20:52:02.6
HOT-2
yeah. oh they weren't giving anything?
20:52:05.6
HOT-1
no.
20:52:05.9
HOT-2
oh.
20:52:07.4
HOT-1
nope they weren't giving anything.
20:52:09.0
HOT-2
jeez.
20:52:10.5
HOT-1
I mean I had a place to stay but you know I'dve still been out of out of uh
income for about ten weeks is what they were calling for.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
205
20:52:18.5
HOT-2
yeah that's— that's really tough.
20:52:34.2
HOT-?
[sound of sniffles]
20:52:39.7
PA-1
folks from the flight deck just to uh give you another update. we're getting
a little bit closer. we're still about number ten for departure. and we'll be
airborne just uh shortly and just to kind of uh pass on a little bit more
information from uh other pilots who have taken off earlier uh the
turbulence has uh decreased uh quite a bit but uh there's still gonna be
some bumps on the climbout so make sure those seatbelts are fastened
tightly. thanks.
20:53:16.7
HOT-2
they're calling winds three hundred at fifteen.
20:53:19.6
HOT-1
three hundred at fifteen.
20:53:43.7
HOT-1
interviewed with Colgan and and uh they gave me the choice of either
going on the nineteen hundred or the Saab. I told them I've flown the
nineteen hundred and it would be a pretty easy transition just learning the
the particular you know profiles and callouts for Colgan as opposed to
Gulfstream. I said but I'd rather have the the Saab so I could learn you
know a little bit more CRM because they have a flight attendant and also
uh I liked the bases better that the Saab had to offer.
20:54:12.1
HOT-2
yeah...yeah.
20:54:23.1
HOT-1
and uh I I was interviewing— have you ever flown with @?
20:54:28.0
HOT-2
nope.
20:54:28.4
HOT-1
do you know who he is?
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
206
20:54:29.3
HOT-2
I know who he is.
20:54:31.1
HOT-1
he uh he was interviewing me along with uh @.
20:54:32.1
HOT-2
**.
20:54:37.0
HOT-2
oh okay.
20:54:37.8
HOT-1
and uh I asked him after the interview. I said you know that's I mean that
was an honest answer but I'd be more challenged in the in the Saab. he
said no man that was a perfect answer. so.
20:54:49.7
HOT-2
oh that's good. well they asked me what I wanted. I said I wanted the Q. I
didn't know much buh difference between the Saab and the Q but um and
they said well tough you can't have it. [sound of laughter] so I was like
why did you ask me if you told me I can't have it? so then they put me in
the Saab I got everything ready we were all set cause we wanted— me
and my husband I mean we lived in Phoenix for a few years we don't
have kids we don't have any commitments. we just you know we wanted
to experience living in different places before we settled back down in
Seattle so we were geared up ready to move to Houston.
20:55:08.7
HOT-1
yeah...yeah go ahead.
20:55:14.9
TWR
attention all aircraft. current altimeter two niner six one.

NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
207
20:55:20.7
HOT-2
uh six one's the altimeter. uh geared up ready to move to Houston. and
then the day before I was supposed to go to training @ called and
basically begged me to switch to the Q and that pushed me back a week
in training and I waited a week and I asked my husband I said look when I
upgrade like thirteen dollars an hour more. it's a bigger plane. I'd rather fly
this plane than the Saab. he says hey we haven't signed anything we
haven't— so we just like switched our whole gears up to Virginia.
20:55:46.6
HOT-1
wow.
20:55:48.9
HOT-2
if they'd told us that all those outstations were gonna close and we'd
come to Newark but but we're ready to be back in Seattle anyway.
20:55:56.1
HOT-1
are you from that area originally?
20:55:58.5
HOT-2
yeah all my family's there. all my husband's family is there. we both grew
up in Seattle. so we want to settle— we want to buy a house with the
market the way it is and I mean it's hard to pass up buying a house right
now.
20:56:06.2
HOT-1
yeah.
20:56:15.0
HOT-2
we * get you know my sister bought a house last year. she thought she
was buying in the bottom of the market and her house has already
decreased thirty thousand dollars in value.
20:56:19.7
HOT-1
uh-huh...dohhh wow.
20:56:24.8
HOT-2
yeah. and we know that that might happen to us too but we're not
gonna— we're not looking to sell in a year or two. we're looking to buy
settle down and live there for you know five to ten years.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
208
20:56:30.0
HOT-1
yeah...it's it's gonna take about that before it uh comes back up. yeah.
20:56:36.8
HOT-2
picks back up.
20:56:40.7
HOT-1
but it's it's got to be close to the bottom if not at the bottom at this point in
time.
20:56:45.8
HOT-2
yeah.
20:56:51.3
HOT-1
yeah I I think— I don't know if it were me if I were buying at this point in
time I think I would start looking about halfway through the year.
20:56:59.7
HOT-2
yeah.
20:57:00.6
HOT-1
halfway or you know into August September time frame.
20:57:04.0
HOT-2
yeah well we're helping my grandpa right now is—. he is a hundred and
he's losing— he doesn't— he's losing his memory. he he can't function.
somebody has to be with him twenty four hours a day. he's not so bad— I
mean if he if he could just— if he couldn't remember who people were all
the time we'd put him in a home.
20:57:23.1
HOT-1
right.
20:57:23.9
HOT-2
but in the morning he's really sharp and then in the afternoon he's got
what's called Sundowner’s it's like part time Alzheimer's.
20:57:29.2
HOT-1
okay.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
209
20:57:29.3
HOT-2
like in the afternoon he starts to go a little- he can't remember. and so my
parents have been going insane. they live next door. they've been having
to be there all the time and my aunts are having to be there. it's so hard
so— while my husband finds a job we've been kind of staying between
my parents house and his house helping out to give them a break. and
then that gives us a break. we're not stuck in a lease for when we find a
house.
20:57:50.7
HOT-1
uh-huh...right.
20:57:54.4
HOT-2
and it— you know it's really nice because everything we're saving goes
straight to a down payment so.
20:58:00.4
HOT-?
[sound of sniffle]
20:58:04.3
HOT-1
yeah I've got a cousin that flies for UPS. he uh flies uh seven fives seven
sixes right seat.
20:58:11.6
HOT-2
yeah.
20:58:11.8
HOT-1
he's in his tenth— or well past his tenth year so he's now in his eleventh
year.
20:58:15.6
HOT-2
yeah.
20:58:18.4
HOT-1
and uh they just sold their house bout uh bout a year ago and they just
bought another house uh and moved into it just at the end of this past
year.
20:58:32.4
HOT-2
yeah.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
210
20:58:33.1
HOT-1
so he he was kind of— he— they sold kind of as the market was going
down.
20:58:38.7
HOT-2
that's good though.
20:58:38.8
HOT-1
they got— they got you know uh something decent out of it. he said he
didn't get quite as much as he could have it he would have sold it you
know six or eight months before.
20:58:49.7
HOT-2
yeah.
20:58:50.1
HOT-1
but um they they didn't lose any money by any means.
20:58:54.8
HOT-2
oh that's good.
20:58:55.7
HOT-1
and uh he got uh it was a house that he said he he had uh put an offer on
and somebody else had already put an offer on which was a lot more
money. and he he said well he could you know it just wasn't worth it to
him.
20:59:14.0
HOT-2
no point in getting into a bidding war in today's market.
20:59:17.8
HOT-1
yeah exactly. and uh the guy's financing did not go through.
20:59:24.1
HOT-2
oh that's nice.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
211
20:59:25.4
HOT-1
and uh you know it's still for sale still for sale still for sale and my cousin
said he called and asked if it you know if it was still for sale or was it still
pending. he said no the financing had had fallen through. so he offered—
uh offered him forty or fifty thousand dollars lower than what they had
offered him at first.
20:59:49.4
HOT-2
yeah.
20:59:49.8
HOT-1
and theirs was already the low offer.
20:59:51.6
HOT-2
yeah.
20:59:51.6
HOT-1
and they got— and they took it.
20:59:53.5
HOT-2
that sucks. oh I mean it's great for your cousin but.
20:59:56.4
HOT
[sound of master caution chime consistent with parking brake application]
20:59:56.5
HOT-1
yeah yeah yeah I mean it sucks for them exactly.
20:59:57.7
HOT-2
yeah.
20:59:59.1
HOT-1
because they were trying— they were trying to get out it. and they were
obviously trying to get the best they could.
21:00:03.0
HOT-2
no of course.
21:00:04.0
HOT-1
just like everybody else does.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
212
21:00:05.4
HOT-2
yeah.
21:00:09.6
HOT-1
ohh wow that guy is— oh we'll see how close this is.
21:00:13.2
HOT-2
ooo...that's not gonna happen.
21:00:23.0
HOT-1
that's a seven two seven just landed. oh that's not too bad. okay.
21:00:28.0
HOT-2
oh yeah 'cause now he just got a thirty knot headwind.
21:00:28.9
HOT-1
*.
21:00:38.2
HOT-2
that wasn't very * it looked a lot closer.
21:00:40.4
HOT-1
yeah it did. it really did.
21:01:11.2
HOT-2
everybody's five.
21:01:29.1
HOT-2
Cargojet?
21:01:31.1
HOT-1
yeah that was that seven two that just—.
21:01:32.3
HOT-2
yeah.
21:01:34.1
HOT-1
Cargojet whoever that is.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
213
21:01:35.4
HOT-2
yeah.
21:02:46.2
HOT-1
Continental fifty. going to Frankfurt.
21:02:59.1
HOT-1
have you guys done very much travelling?
21:03:01.1
HOT-2
um-hmm.
21:03:01.7
HOT-1
oh good.
21:03:02.9
HOT-2
yeah we— my husband goes to— he was going to Phoenix almost every
month. when he drilled there. he drilled once a month there.
21:03:10.2
HOT-1
uh-huh.
21:03:10.9
HOT-2
and uh he just got based back in Seattle which is nice because he make
more in one weekend of drill than I make in an entire pay cycle here.
21:03:19.6
HOT-1
that sucks. what branch is he with?
21:03:20.3
HOT-2
well he's army.
21:03:23.1
HOT-1
army.
21:03:23.1
HOT-2
uh that'll hopefully change now I— the next paycheck that comes should
have my five dollar raise on it.
21:03:30.3
HOT-1
good.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
214
21:03:30.8
HOT-2
I thought the last one should because I got hired January sixteenth. but
apparently the sixteenth through the thirtieth they said that you don't get
your raise until the pay period after.
21:03:39.3
HOT-1
it would be the twentieth.
21:03:40.7
HOT-2
yeah that made me— but but no— but my but my pay from the sixteenth
to the thirtieth didn't have the raise in it.
21:03:46.1
HOT-1
uh-huh.
21:03:47.6
HOT-2
and I got hired on the sixteenth.
21:03:48.8
HOT-1
that's okay. it'll it'll be retroed back.
21:03:50.8
HOT-2
no no she said it wouldn't. I called and asked.
21:03:53.1
HOT-1
why wouldn't it be retroed back?
21:03:54.1
HOT-2
because she says that your raise doesn't take effect until the first pay
period— the first full pay period after you got hired. so I got hired on the
sixteenth and the pay period started on the sixteenth. so from the
sixteenth to the thirtieth that my raise wasn't in effect until after that. I'm
thinking that's like two hundred buck— two hundred bucks to an FO is a
lot of money.
21:04:12.6
HOT-1
ohhh I think I'd question that.
21:04:15.0
HOT-2
I did. and she— and I called payroll and they said that that's just how
policy is.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
215
21:04:23.7
HOT-2
so I talked to two different people. I talked to payroll and they gave me
someone from HR and that's what it— both of them said that and I
thought that was a load of crap.
21:04:30.0
HOT-1
okay oh that's not the way they used to do it. that may be how Pinnacle
does it.
21:04:35.1
HOT-2
yeah but.
21:04:36.7
HOT-1
that's not how Colgan used to do it.
21:04:39.1
HOT-2
no but I'll be getting an extra two hundred dollars each paycheck. now I'll
be making more than he does in a weekend but.
21:04:45.1
HOT-1
[sound of laughter]
21:04:45.5
HOT-2
[sound of laughter] that's good.
21:04:50.6
HOT-2
oh.
21:04:54.1
HOT-1
what was it?
21:04:55.2
HOT-2
is it a Bell?
21:04:56.3
HOT-1
I don't know. kind of looked like it didn't it.
21:04:58.5
HOT
[sound of master caution chime consistent with parking brake application]
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
216
21:04:59.4
HOT-2
yeah.
21:05:01.0
HOT-1
well this isn't an elephant so I'm not scared of it.
21:05:03.9
HOT-2
yeah that's for sure. no but we uh we travelled to Phoenix a lot and 'cause
we used to live there and he went down to— we went to Disneyworld and
now that we're back in Seattle— we've got two dogs. so now that we're
back in Seattle with all of our family it's a lot easier to just take off and you
know my sister can wake up in the morning and find two extra dogs in her
backyard. [sound of laughter]
21:05:24.7
HOT-1
right.
21:05:36.0
HOT-?
[sound of sniffle]
21:05:37.2
HOT-1
that's what uh my wife and I did before we— you know settled down and
had you know bought a house and had you know started a family and all
that kind of stuff. we uh wanted to get to know each other more and more
and you know just enjoy the time between the two of us. because you
know obviously when you start a family and everything and it's just not the
same. it's just you're closing one chapter or one book and opening
another.
21:05:53.8
HOT-2
yeah...exactly.
21:05:58.7
HOT
[sound of master caution chime]
21:06:05.1
HOT-1
uh but we I mean we always fit our children into our schedule and uh you
know and also you know focused on their schedules too to make a
compromise. it wasn't all one sided. it wasn't all for the kids it wasn't all for
us but uh we didn't let their lives run ours.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
217
21:06:19.3
HOT-2
yeah...that's good.
21:06:31.9
HOT-1
and you know that's that's the big thing that I'd I'd recommend to any
young couple that's that's out there just unsolicited advice you know just
you know don't get in a big hurry.
21:06:43.5
HOT-2
yeah. no we're not. we want to give it— we want to do a lot more
travelling. although gosh I'm so freaking mad. I feel like Colgan walks all
over me. this company treats me like crap so much. I've been assigned
my vacation in March. and I have been— I have sent four emails and I've
made a dozen calls saying I do not want vacation in march I never
requested that. that was assigned to me. here are ten different other
weeks that I'd like vacation that are open on the vacation slot and she
won't give it to me. she won't give it to me. I've called @. she's the one
dealing with it. I've left her voicemails she won't call me back. I've sent her
emails she won't call me back. she won't change my vacation. it still even
has me in Norfolk she won't change it. and I think I've got like two more
days before I'm within the forty five days and they can't change it. and I
know she's going to screw me over and I'm going to be so freaking mad if
they make me take my vacation in march cause I can't— I don't want to
take vacation when my husband can't take vacation because we want to
go somewhere.
21:07:17.2
HOT-1
sh— um...right right.
21:07:39.4
HOT-1
um now that she she looks at it on the tenth of every month and then
posts it right after that so take a look.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
218
21:07:46.1
HOT-2
but I— I did I did she just emailed me she said you can't have Christmas
off. and I said but what about the other ten weeks I asked for off you know
and she did— she wouldn't email me back and it's just like— I if I only get
to bid one week every month the entire year's gonna go by without me
being able to get a bid in. because if somebody else higher than me
wants that week off and she she and she won't respond back the fact that
I'm in Newark now and I had to wait until I was in Newark to make my bid
that's what I waited ‘til uh two months ago is when I started you know
getting to do it. she won't do anything to help me and it's like I don't know
what to do and I'm just gonna get screwed into having— I mean I literally
have sent like several emails made several phone calls—.
21:07:58.1
HOT-1
ah.
21:08:27.1
HOT-1
go to @. that's what he's there for.
21:08:29.7
HOT-2
is it?
21:08:30.1
HOT-1
yeah oh hell yeah. oh yeah.
21:08:32.1
HOT-2
because I just— you know I can't get walked on anymore.
21:08:35.6
HOT-1
oh no. go to @ and just say look you know.
21:08:38.6
HOT-2
I don't want— yeah.
21:08:40.1
HOT-1
you know you don't want to piss anybody off. you don't want to make—
you don't—.
21:08:42.1
HOT-2
no and I have been very polite about it. I haven't— I haven't gotten angry.
I haven't you know—.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
219
21:08:47.9
HOT-1
just just like you just told me. you feel like you're getting walked all over.
21:08:51.5
HOT-2
oh yeah.
21:08:52.1
HOT-1
and there's no reason for it. and you looked on the on the spreadsheet
and there's weeks available and everything?
21:08:56.3
HOT-2
and I sent her— and there's weeks available. and I sent her like— I sent I
want you know I said if I can't have Christmas what about— I said I want
Christmas I know that ones probably full. I'd like then the week after and
then if that one's full the week before Christmas. if that one's full then
Thanksgiving and then I went through I said if I can't have any of that I
would like any week available after may. and she wouldn't give me any—
there's got to be a week available after May.
21:09:19.3
HOT-1
well you can check and see if there's weeks available.
21:09:21.5
HOT-2
I did and all those weeks that I said— the only week that was filled was
Christmas week. the week after was open. the week before was open and
she wouldn't give me any of those. she only— she only responded saying
that Christmas week was full. she didn't respond to any of the other— I
can't get her to respond to me. she wouldn't tell me that any of the other
weeks were full. she wouldn't sign me up for any of the other weeks and
I'm still scheduled for vacation in March.
21:09:41.9
HOT-1
okay uhh.
21:09:44.9
HOT-2
but I'll give her a call again tomorrow and I haven't checked any of my
emails.
21:09:47.6
HOT-1
but she's— yeah she's not gonna look at uh vacation again basically until
the tenth of next month.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
220
21:09:53.5
HOT-2
so that that means I'm screwed and I just have to have it in march 'cause
the tenth of March.
21:09:57.4
HOT-1
no no go to @.
21:09:59.1
HOT-2
yeah I mean that's the thing I told her you know like if she waits ‘til the
tenth of march that's gonna be after you know after March bids are
already— they'll have you know they'll have already given me vacation for
March.
21:10:14.8
HOT-1
oh yeah yeah I see what you're saying.
21:10:17.0
HOT-2
so I can't you know I can't wait ‘til—.
21:10:19.8
HOT-1
okay yeah go to @.
21:10:21.3
HOT-2
yeah.
21:10:23.5
HOT-1
it it's been— what I would do before you go to @ is look up your FO
vacation spreadsheet. print it.
21:10:31.7
HOT-2
um-hum...yeah yeah.
21:10:33.3
HOT-1
and say okay well you know this is— and and if you still have a copy of
your email. print it. this is what I've done so far and highlight the the
spaces that are still available and and it doesn't matter whether you're
based in Newark or Norfolk or or Albany.
21:10:35.3
HOT-2
yeah...um-hum...yeah...well sh— well if I was based—.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
221
21:10:50.9
HOT-1
cause every— everything on the Q is on the Q. everything on the Saab is
on the Saab.
21:10:57.1
HOT-2
um-hum.
21:10:58.2
HOT-1
they don't do it by base anymore.
21:11:00.3
HOT-2
oh I thought— that what she emailed me back. she said only two FOs per
base can have each week off. but then there are some weeks—.
21:11:07.6
HOT-1
well that's funny 'cause there's five captains that uh that are you know that
out of five captains four of them are from Newark one's from Norfolk *.
21:11:19.8
HOT-2
exactly.
21:11:21.2
HOT-1
you know it's like *.
21:11:23.4
HOT-2
and then if they do it that way then who doesn't get vacation? because
there's more than fifty two FOs.
21:11:28.9
HOT-1
because— and here's another thought. or here's another 'nother deal with
that—.
21:11:32.7
HOT-2
or a hundred four FOs.
21:11:34.2
HOT-1
um then then you should have been given the vacation of your choice if
you're based in Norfolk if they're if they're separating it.
21:11:43.6
HOT-2
yeah.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
222
21:11:43.7
HOT-1
and the only people that you'd be competing with would be Norfolk based
FOs.
21:11:47.6
HOT-2
yeah but now I'm—.
21:11:48.6
HOT-1
likewise Albany and stuff like that.
21:11:51.5
HOT-2
yeah.
21:11:53.6
HOT-1
but uh yeah I would just uh I would go to @ at this point.
21:11:59.0
HOT-2
yeah cause I can't wait— I mean I tried— I sent her very polite very nice
emails. I haven't been like this upset at her. I just— you know I've sent her
nice polite emails. I cannot wait. I do not want to have vacation in march.
I've been telling you this for two months. I don't want my vacation in
march. I do not want to get stuck with having it— having to take it. ‘cause
it's not within forty five days.
21:12:20.8
HOT-1
right.
21:12:21.7
HOT-2
I mean I've never had a company be like this before with vacations.
21:12:38.7
HOT-2
why can't we take off two two right?
21:13:47.1
HOT-?
[sound of sniffle]
21:13:48.1
HOT-2
my husband look at my email. I haven't looked for two days. I emailed her
and then I— and then it was two days before—.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
223
21:14:27.0
HOT-1
not much on the departure roll.
21:14:29.6
HOT-2
what?
21:14:30.3
HOT-1
said not much on the departure roll. he ain't rollin' too fast.
21:14:33.5
HOT-2
uh-uh.
21:14:37.3
HOT-1
**.
21:15:00.5
HOT-1
wow.
21:15:50.8
HOT-1
let's do a taxi checklist.
21:15:52.3
HOT-2
alrighty. taxi checklist. takeoff data briefing set complete.
21:15:55.4
HOT-1
set complete.
21:15:56.1
HOT-2
condition levers max?
21:15:57.3
HOT-1
max.
21:15:57.8
HOT-2
trims three set.
21:15:58.9
HOT-1
three set.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
224
21:15:59.4
HOT-2
and takeoff warning?
21:16:00.4
HOT-1
test.
21:16:00.8
HOT-2
taxi check complete.
21:16:06.5
HOT-2
and we're following JetBlue.
21:16:09.4
HOT-1
well for the time being anyway.
21:16:11.0
HOT-2
yeah *.
21:16:12.1
HOT-1
unless they cut us off...which is entirely possible.
21:16:23.4
HOT-1
slide right. leave a little room.
21:16:25.3
HOT-2
what?
21:16:25.9
HOT-1
** give these guys a little room here.
21:16:28.6
HOT-2
yeah.
21:16:29.3
HOT-1
JIC. just in case.
21:16:31.7
HOT
[sound of master caution chime]
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
225
21:16:50.6
HOT-1
well.
21:16:58.2
HOT-1
I'll take it.
21:17:00.3
HOT-2
yeah me too.
21:17:05.9
PA-2
folks it looks like we're number two for departure. should be pretty quick
here. like to have the flight attendants please take their seats. thank you.
21:17:22.6
TWR
Colgan thirty four oh seven on uh departure you're gonna turn— fly
heading two seven zero maintain two thousand now.
21:17:30.1
RDO-1
two seven zero maintain two thousand Colgan thirty four oh seven.
21:17:30.7
HOT-2
oh.
21:17:38.3
HOT-1
alright heading two seven zero.
21:17:41.8
HOT-2
and it's still five thousand?
21:17:42.9
HOT-1
and two thousand.
21:17:44.0
TWR
Colgan thirty four oh seven runway two two right at whiskey.
position and hold.
21:17:47.2
RDO-2
position and hold Colgan thirty four oh seven.
21:17:49.9
HOT-1
alright pos and hold. before takeoff checklist.

NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
226
21:17:55.7
HOT-2
uh before takeoff checklist. watch your legs. FA notification received
transponder TCAS on ALT flight control checked free radar terrain off.
flight taxi flight. cabin PA complete. external lights on. before takeoff
checklist complete.
21:18:18.9
HOT-2
okay.
21:18:22.8
TWR
and Colgan thirty four oh seven runway two two right at whiskey
winds three zero zero at one niner cleared for takeoff.
21:18:27.7
RDO-2
cleared for takeoff Colgan thirty four zero seven.
21:18:30.3
HOT-1
alright cleared for takeoff it's mine up to two thousand heading two seven
zero after departure. here we go.
21:18:35.4
CAM
[sound of increasing engine rpm]
21:18:42.3
HOT-1
check power.
21:18:44.6
HOT-2
and power checked.
21:18:48.8
HOT-2
eighty knots.
21:18:50.1
HOT-1
eighty.
21:18:55.0
HOT-2
V one.
21:18:56.2
HOT-2
rotate.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
227
21:19:01.6
HOT-2
positive rate.
21:19:02.3
HOT-1
gear up.
21:19:03.0
CAM
[sound similar to landing gear handle movement]
21:19:07.5
CAM
[sound similar nose gear uplock and door closing]
21:19:10.4
TWR
Colgan thirty four oh seven turn right heading two seven zero
maintain two thousand contact New York Departure.
21:19:15.0
RDO-2
right two seventy two thousand and over to departure Colgan thirty
four zero seven.
21:19:20.7
RDO-2
Departure Colgan thirty four oh seven is seven hundred for two
thousand heading two seventy.
21:19:26.5
DEP-A
Colgan uh thirty four oh seven New York radar contact. climb
maintain one zero ten thousand.
21:19:31.6
HOT
[sound similar to altitude alert]
21:19:32.5
RDO-2
up to ten thousand Colgan thirty four zero seven.
21:19:35.5
HOT-2
ten thousand.
21:19:36.4
HOT-1
ten thousand alt sel flaps zero. set indicated airspeed two ten. climb
checklist.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
228
21:19:44.3
HOT-2
alrighty.
21:19:45.4
CAM
[sound similar to decreasing propeller rpm]
21:20:08.9
DEP-A
Colgan thirty four oh seven proceed direct COATE.
21:20:11.5
RDO-2
direct COATE Colgan thirty four zero seven.
21:20:13.9
HOT-2
direct COATE.
21:20:14.2
HOT-1
direct COATE.
21:20:19.5
HOT-1
and NAV for me.
21:20:20.2
HOT-2
NAV selected.
21:20:39.9
HOT-1
wee this is fun.
21:20:41.7
HOT-2
yeah.
21:20:43.0
HOT-1
okay almost.
21:20:46.6
DEP-A
Colgan thirty four oh seven contact departure one one eight one
seven. eighteen seventeen.
21:20:50.9
RDO-2
eighteen seventeen Colgan thirty two— thirty four zero seven.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
229
21:21:00.9
RDO-2
[sound of mic click]
21:21:10.0
RDO-2
departure Colgan thirty four zero seven five point seven for ten
thousand.
21:21:14.2
DEP-B
Colgan thirty four zero seven New York Departure roger.
21:22:27.0
HOT-2
and climb checklist complete. I don't know if I said it or not.
21:22:31.0
PA-3
ladies and gentlemen for your continued safety we do ask that you keep
your seatbelts securely fastened even if the captain turns off the fasten
seatbelt sign. we would like to add a special welcome to our One Pass
members. you'll be earning valuable miles for your trip today. if you are
not already a member of the One Pass program you can enroll online at
Continental dot com...Continental Connection is pleased to provide you
with a complimentary copy of Sky Mall catalogue and Continental
Magazine both located in your seat pocket.
21:22:31.6
HOT-1
autopilot's engaged.
21:22:33.5
HOT-2
alright.
21:22:39.2
HOT-1
it's probably a good thing.
21:22:43.7
HOT
[sound similar to altitude alert]
21:22:44.9
HOT-1
nine ten alt sel.
21:22:45.7
HOT-2
ten alt sel.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
230
21:23:08.7
HOT
[sound of double chime]
21:23:14.1
PA-2
we're through ten thousand feet.
21:23:24.3
PA-3
ladies and gentlemen the use of approved portable electronic devices is
now permitted.
21:23:56.6
DEP-B
Colgan thirty four zero seven climb maintain one two twelve
thousand. proceed direct COATE.
21:24:01.4
RDO-2
twelve thousand direct COATE Colgan thirty four zero seven.
21:24:04.6
HOT-1
twelve alt sel.
21:24:05.4
HOT-2
twelve alt sel.
21:24:18.4
HOT-?
[sound of sniffle]
21:24:47.2
HOT-1
eleven twelve alt sel.
21:24:47.3
HOT
[sound similar to altitude alert]
21:24:48.6
HOT-2
eleven twelve alt sel.
21:25:14.2
HOT-1
have you ever looked at the logbook very much as far as uh like putting
your times and stuff in?
21:25:19.8
HOT-2
um-hum.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
231
21:25:20.7
HOT-1
* okay. I kinda * you just haven't done like writeups?
21:25:25.2
HOT-2
yeah I just haven't written anything in it but I've looked at it and looked up
crew writeups.
21:26:18.0
HOT-1
well I didn't write any numbers down so.
21:26:21.8
HOT
[sound of double chime]
21:26:23.6
HOT-1
uh.
21:26:24.8
INT-2
hello.
21:26:25.6
INT-3
hi what do you think about doing service?
21:26:29.0
INT-1
actually I think if you could uh do something fairly quick I think we might
be okay. I don't have a whole lotta cloud cover up here.
21:26:36.4
INT-3
okay.
21:26:37.1
INT-1
uh just be careful.
21:26:38.8
INT-3
okay.
21:26:39.1
INT-1
if we hear of anything—.
21:26:40.7
INT-3
give us a buzz.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
232
21:26:41.2
INT-1
we will.
21:26:41.9
INT-3
alright thanks.
21:27:08.1
DEP-B
Colgan thirty four zero seven contact New York Center one tree two
point six good day.
21:27:12.6
RDO-2
one three two point six Colgan thirty four zero seven.
21:27:22.4
RDO-2
departure Colgan thirty four zero seven twelve thousand direct
COATE.
21:27:29.3
HOT-1
geez.
21:27:30.7
HOT-1
this I **.
21:27:31.5
ZNY-A
Colgan thirty four zero seven New York Center you should be with
the New York Center on one three two point six.
21:27:40.8
RDO-2
alrighty we'll try them thirty four zero seven thanks.
21:28:12.9
RDO-2
Center Colgan thirty four zero seven twelve thousand direct
COATE.
21:28:16.8
ZNY-B
Colgan thirty four zero seven New York Center roger. Wilkes-Barre
altimeter two nine six seven.
21:28:22.3
RDO-2
six seven thanks.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
233
21:28:25.1
HOT-2
six seven.
21:28:25.6
HOT-1
sixty seven set crosscheck.
21:28:27.4
HOT-2
set crosschecked.
21:28:30.1
HOT-1
alright.
21:28:42.0
HOT-1
today's the twelfth right?
21:28:43.5
HOT-2
yup.
21:28:47.0
HOT-2
at least that's what you told me earlier.
21:28:50.2
HOT-1
well that's my story and I'm sticking to it.
21:28:52.2
HOT-2
alright.
21:28:58.5
HOT-1
well that's good.
21:29:19.7
HOT-1
so where's this page here? I don't see any writing on it.
21:29:32.6
HOT-1
interesting.
21:29:46.0
HOT-?
[sound of throat clearing]
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
234
21:29:50.1
HOT-1
alright I'll give that to you.
21:29:52.8
HOT-2
alright.
21:29:53.7
HOT-1
fill out what you can...I'll sign it **.
21:30:31.1
HOT-2
it's Zulu time is the in and out right?
21:30:34.3
HOT-1
uh that's in Zulu time but we want it local time.
21:30:36.3
HOT-2
yeah local okay.
21:30:38.5
HOT-1
on here. so just minus five. sooooo let's see.
21:30:45.4
HOT-2
so nineteen forty five.
21:30:47.5
HOT-1
seven forty five yeah nineteen forty five...wow an hour and a half taxi.
21:30:53.7
HOT-2
yeah. **.
21:30:57.8
HOT-1
oh that just— that just stinks...we can't reap the benefit.
21:31:04.3
HOT-2
I know.
21:31:18.1
RDO-1
blocked.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
235
21:31:44.6
ZNY-B
Colgan thirty four zero seven climb to flight level— correction climb
to one six thousand.
21:31:50.0
RDO-2
one six thousand Colgan thirty four zero seven.
21:31:53.0
HOT-2
sixteen.
21:31:53.5
HOT-1
sixteen alt sel.
21:31:54.9
HOT-2
alt sel.
21:32:08.4
HOT-1
oops. you didn't feel that.
21:32:11.0
HOT-2
no I didn't feel that.
21:32:13.0
HOT-2
they didn't do a twenty four hour ice protection test.
21:32:15.4
HOT-1
yeah I just did.
21:32:16.5
HOT-2
you did?
21:32:17.2
HOT-1
yup.
21:32:20.5
HOT-1
that's why I was looking back on all those pages.
21:32:22.8
HOT-2
yeah.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
236
21:32:23.2
HOT-1
it said it was miss— er uh you know.
21:32:27.3
HOT-2
yeah.
21:32:28.0
HOT-1
there uh there was one page there wasn't anything on it. so it's like they
they tore it out in error.
21:32:34.1
HOT-2
oh yeah.
21:32:35.4
HOT-1
so.
21:32:58.1
HOT-2
just twenty four ice test complete? or write—.
21:33:02.0
HOT-1
yeah I'd— I'd put twenty four hour uh check's complete.
21:33:19.1
HOT-2
alrighty.
21:33:20.9
ZNY-B
Colgan thirty four zero seven contact New York Center one tree tree
point tree five.
21:33:25.8
RDO-2
one three three point three five Colgan thirty four zero seven.
21:33:31.8
HOT-1
there we go.
21:33:32.9
RDO-2
thirty four zero seven fourteen point one for sixteen thousand.
21:33:37.3
ZNY-C
Colgan thirty four zero seven New York Center roger. Wilkes-Barre
altimeter two niner six seven.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
237
21:33:42.4
RDO-2
six seven thank you thirty four oh seven.
21:33:48.0
HOT-2
I'm assuming we're only gonna land once.
21:33:51.6
HOT-1
yeah.
21:33:56.8
HOT-1
the only thing that um I would not do— well the type of flight— I don't
know if you can see it here. I'll show you.
21:34:03.8
HOT-2
I see. oh yeah I didn't know what to—.
21:34:05.9
HOT-1
if if you don't know the type of flight it is it's— it's down here on the
bottom.
21:34:08.1
HOT-2
uh-huh. oh oh okay.
21:34:10.2
HOT-1
just a regular revenue flight—.
21:34:11.4
HOT
[sound similar to altitude alert]
21:34:12.3
HOT-1
fifteen sixteen alt sel. regular revenue flight is type one.
21:34:15.2
HOT-2
okay.
21:34:17.3
HOT-1
unless it's a reposition or special ferry or whatever it's something else.
21:34:21.0
HOT-2
[sound of sneeze]
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
238
21:34:21.6
HOT-1
bless you.
21:34:22.2
HOT-2
excuse me. okay.
21:34:24.0
HOT-1
um a— and this is just my little deal and it is what I was taught and
everything. and and it makes sense to me.
21:34:31.9
HOT-2
sure.
21:34:32.7
HOT-1
um on your two.
21:34:35.6
HOT-2
uh-huh.
21:34:36.3
HOT-1
what happens if we have to divert to an alternate?
21:34:39.0
HOT-2
oh yeah that's true.
21:34:40.0
HOT-1
um I was told it was their little uh uh like superstition.
21:34:46.3
HOT-2
oh.
21:34:46.6
HOT-1
you don't put— you don't put it until you land there.
21:34:49.3
HOT-2
right right. no that makes sense.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
239
21:34:49.7
HOT-1
uh but well okay. well you can take it that far. I don't care. but it makes
sense that if you have to divert someplace at least you're not scratching
through and doing all that kind of stuff. uh but I still do the one landing and
however many starts we have and fill the rest of it out.
21:34:59.3
HOT-2
yeah.
21:35:06.5
HOT-2
yeah.
21:35:07.9
HOT-1
but uh other than that that's all there is to it. on your writeups—.
21:35:15.0
HOT-2
I've written— I mean I've written other planes up before. just not from—
with Colgan.
21:35:18.1
HOT-1
okay alright so you know like the one P or the two P as you write ‘em up
like that?
21:35:20.6
HOT-2
uh-huh. yeah.
21:35:23.7
HOT-1
write it up. uh and if you're doing one twenty one ops you obviously know
as short sweet to the point as you possibly can um.
21:35:36.0
HOT-2
give em all the details that you need to give.
21:35:38.2
HOT-1
yeah but but also don't get too wordy with it.
21:35:42.4
HOT-2
right.
21:35:44.0
HOT-1
um and what I try to do is— is I'd look up in the MEL book.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
240
21:35:54.7
HOT-2
uh-huh.
21:35:55.3
HOT-1
to begin with before I write things up.
21:35:58.0
HOT-2
so you know yeah.
21:35:59.0
HOT-1
that way if I screw up and write it up one way and it grounds the airplane
but it's not— it's not exactly or I could write it up slightly different to get an
MEL to get it back to where you can do maintenance type of deal.
21:36:15.1
HOT-2
yeah.
21:36:16.3
HOT-1
it's it's a judgment call by all means.
21:36:19.7
HOT-2
yeah.
21:36:21.2
HOT-1
you you definitely want to write the proper thing up. um you know I try to
uh uh get em to fix— I uh on the Saab we don't have glass we uh we had
EFIS screens.
21:36:37.7
HOT-2
right.
21:36:40.1
HOT-1
but uh you had a EHSI and uh a EADI.
21:36:45.5
HOT-2
uh-huh.
21:36:46.2
HOT-1
I wrote up the course selector. course one selector.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
241
21:36:49.0
HOT-2
uh-huh.
21:36:50.7
HOT-1
uh because it wouldn't move. it was stuck on one particular course
setting.
21:36:55.9
HOT-2
uh-huh.
21:36:56.7
HOT-1
and uh wrote it up totally explained exactly what it was and they uh at the
time there were four planes down. two getting line checks and then my
airplane and another one uh that had something wrong with it. they only
had four mechanics on duty at the time. so they were all trying to do
something. er I'm sorry they had four down I was the fifth one.
21:37:20.1
HOT-2
oh okay.
21:37:21.1
HOT-1
so they tried to MEL the uh the uh the autopilot system uh because of the
heading selector.
21:37:32.0
HOT-2
yeah.
21:37:32.6
HOT-1
I you know I wouldn't be able to turn. and it's like wait a minute. it doesn't
even apply.
21:37:36.4
HOT-2
yeah.
21:37:37.4
HOT-1
so uh you got to be careful about that.
21:37:40.5
HOT-2
yeah.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
242
21:37:41.2
HOT-1
just don't— you know understand the MELs that they uh they try to put on
it make sure it applies to what you're doing.
21:37:48.3
HOT-2
yeah.
21:37:48.7
HOT-1
and the problem you're having. and I I called ‘em back and told ‘em uh
that it doesn't have anything to do with the autopilot. well I mean doesn't it
do this this this? no it's— this is what's wrong or this is what I told them
before. ohhhhhh.
21:38:03.6
HOT-2
yeah.
21:38:04.6
HOT-1
ehh well can we just go ahead with that MELed we'll uh get it—. well I'll
tell you we could go with that MEL but I can't sign the release. I guess
we'll have to get somebody to fix it then won't we. well I guess we will.
21:38:18.9
HOT-2
[sound of laughter]
21:38:19.5
HOT-1
took em twenty minutes to fix it. they just had to pop out a panel uh little
component put in another component.
21:38:25.2
HOT-2
yeah.
21:38:26.1
HOT-1
and it took em all of twenty minutes. it's just the fact that they were
shorthanded.
21:38:29.2
HOT-2
oh yeah.
21:38:29.7
HOT-1
they were trying to uh uh—.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
243
21:38:31.9
HOT-2
save a minute here.
21:38:32.7
HOT-1
yeah save a minute here. get us out back and then they would have time
to do it.
21:38:36.8
HOT-2
yeah.
21:38:41.1
HOT-1
but of course that turned into a fiasco. we were going to Alexandria
Louisiana that night.
21:38:46.3
HOT-2
oh yeah.
21:38:46.7
HOT-1
and uh let's do a cruise checklist.
21:38:49.8
HOT-2
oh cruise checklist.
21:38:51.2
HOT-1
yeah.
21:38:52.4
HOT-2
altimeters two niner six seven set crosscheck.
21:38:54.9
HOT-1
two niner six seven set crosscheck.
21:38:57.5
HOT-2
power set seatbelt sign on lights set cabin pressure check. and well cabin
pressure. what's Buffalo at?
21:39:07.0
HOT-1
uh not too much. uh seven twenty eight.
21:39:08.7
HOT-2
seven hundred.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
244
21:39:12.7
HOT-2
cabin pressure check and twenty four hour ice protection test complete.
cruise checklist complete. um-huh.
21:39:17.2
HOT-1
thanks. yeah we uh after they fixed it so— we were already delayed. they
fixed it we were delayed a little bit more. no big deal.
21:39:24.0
HOT-2
yeah.
21:39:24.2
HOT-1
get in uh start up number two and we're doing the paperwork and all of a
sudden we get bing. look— it looked— it was engine lookup light. I went
oh crap that's not good. I looked up it was chip detect. right chip detect.
21:39:43.3
HOT-2
what's that?
21:39:43.7
HOT-1
what— what that— what that's doing is detecting chips of metal in the
engine.
21:39:48.4
HOT-2
oh.
21:39:50.2
HOT-1
and uh we were thinking aww crap. so I said grab the checklist real quick
and let's just go through it. well in the chip detect abnormal checklist
there's nothing pertaining to on the ground. it's all pertaining to in the air
so I said okay shut it down. called maintenance they came over they
cleaned out a little filter screen. they said it was probably carbon built up
blah blah blah.
21:40:05.3
ZNY-C
two eight charlie golf climb and maintain flight level two two zero.
21:40:09.8
N28CG
two zero zero for two two zero two eight charlie golf.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
245
21:40:12.1
ZNY-C
and how would you describe the icing?
21:40:16.8
HOT-2
yeah.
21:40:17.4
HOT-1
they fel— uh cleaned out this little carbon screen. did uh a runup check
observation. I kept everybody on the plane. told em what was going on.
man their eyes were you know they're all over here watching what they
were doing. but it was either that or they'd have to get bussed around get
out and bout the time that they'd get out they would bus em back around.
21:40:18.3
N28CG
yeah we'll call it about light to moderate rime.
21:40:36.7
HOT-2
yeah.
21:40:37.2
HOT-1
anyway we started up ops check good. so filling out filling out the
paperwork. got the door closed and everything. it's got a little whiskey
hatch over here.
21:40:45.4
HOT-2
uh-huh.
21:40:46.0
HOT-1
I'm handing the paperwork out. ding. #. right chip detect— chip detect
again.
21:40:51.8
HOT-2
ohh.
21:40:52.8
HOT-1
so I shut it down told everybody yeah we're gonna have to get another
airplane. they had another airplane it was on a Saturday so they had
extra— they had spares because of the schedule and everything.
21:41:01.9
HOT-2
yeah.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
246
21:41:04.4
HOT-1
um so uh twenty minutes later we launch and get about halfway up there
uh over this one VOR and uh all of a sudden oh and uh uh I'll back up a
half a step. I was telling the—telling the FO this was like— I don't know a
month after I upgraded to captain.
21:41:29.7
HOT-2
oh geez.
21:41:30.6
HOT-1
I said you know uh uh all this stuff is just happening to me. and it's— you
know hell the only thing I haven't had is is an air return.
21:41:39.8
HOT-2
oh God.
21:41:40.8
HOT-1
so we get over this VOR headed to Alexandria. ding ding ding. that's not a
caution light that's a master warning.
21:41:48.5
HOT-2
yeah.
21:41:50.5
HOT-1
and uh looked up avionics smoke detector.
21:41:56.2
HOT-2
ohh.
21:41:58.2
HOT-1
I'm going @ my FO cool as #. man should I get my uh smoke goggles on
and everything. said yeah gimme— gimme the memory items. I'm— I'm
over here. I don't smell anything. the avionics bay is right behind the
captain's seat.
21:42:15.9
HOT-2
yeah.
21:42:17.1
HOT-1
there's a little uh fire bottle. little uh rubber kind of cover thing that you can
stick the fire bottle into and blow it if you need to if you're actually on fire.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
247
21:42:21.1
HOT-2
uh-huh...uh-huh.
21:42:28.2
HOT-1
I reach back in here and find it and uh I open it up because it's— it's kind
of like a drainer in a sink.
21:42:35.5
HOT-2
yeah.
21:42:35.9
HOT-1
like over a garbage disposal. it's just kinda like this. and it's rubber and
you can push.
21:42:40.2
HOT-2
uh-huh.
21:42:40.5
HOT-1
so I pushed it. man man I don't smell anything. called the flight attendant.
@ hey do you smell any smoke back there? no. why? should I?
21:42:53.3
HOT-2
[sound of laughter]
21:42:55.5
HOT-1
well no you shouldn't. I'm glad you don't. thanks for playing the game.
and— and I just cut her off. good *. [sound of laughter]
21:43:04.3
HOT-2
nice.
21:43:05.9
HOT-1
she calls back well uh what— what do you want me to do? I said naw
man uh I said I think it's just a false alarm. but uh I was just checking. we
just— we've got a light up here that went off. I said I don't think there's
anything to it. so anyway she— she was good with that. and uh we didn't
have ACARS— we don't have ACARS in the Saabs. so I called uh
Manassas on ARINC. I said uh so uh what do you want me to do? go
back to Houston? continue on or what? call us when you get on the
ground in Alexandria. hey no problem. so they're gonna do a road trip and
change the smoke detector out.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
248
21:43:23.7
HOT-2
yeah...yeah.
21:43:48.5
HOT-1
and uh sure enough by the next morning— we were taking it out the next
morning they had— they had come— they did a road trip from Houston.
changed the deal out. away we went. of course after that day uh we all
went to the uh steakhouse. we ate a steak baked potato and drank a
messload of beer.
21:44:09.4
HOT-2
yeah.
21:44:10.2
HOT-1
it was just one of those— one of those days. yeah.
21:44:12.1
HOT-2
one of those days where you have to have a few beers at the end.
21:44:16.4
HOT-1
that was that was a good time. I like flying the Saab. if— if you upgrade to
the Saab— I mean if you have the opportunity to upgrade to Saab versus
the Q and you want to get your PIC time.
21:44:29.2
HOT-2
um-huh.
21:44:29.5
HOT-1
and uh you know and if that's uh you know a goal for you I guess go
ahead and do it.
21:44:34.0
HOT-2
yeah. um-huh.
21:44:35.8
HOT-1
that a neat airplane to fly. it's not like this.
21:44:38.2
HOT-2
yeah right.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
249
21:44:40.1
HOT-1
I mean it's taking five steps backwards but you're in the left seat.
21:44:46.2
HOT-2
yeah.
21:44:46.5
HOT-1
it's— it's like moms SUV or minivan. you know the soccer van uh you
don't have to fly with your hands and your feet. you just fly with your
hands.
21:44:59.2
HOT-2
yeah.
21:44:59.5
HOT-1
once you— once you flip the auto— uh the yaw damp on and autopilot on
it's solid as a rock.
21:45:05.2
HOT-2
works the rudders for you.
21:45:07.1
HOT-1
yeah it works rudders for you. it's all coordinated.
21:45:09.9
HOT-2
I think it's fun flying with— with captains. not so much any— lately but
right at first that came from the Saab and they'd see— they'd see the
rudder and they'd— aww # and kick it really hard and fling the plane back
and forth.
21:45:23.8
HOT-1
kind of like I did a little while ago.
21:45:25.4
HOT-2
yeah kind of but uh at first I flew— I flew with some captains that were
doing it really bad.
21:45:30.5
HOT-1
really.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
250
21:45:30.9
HOT-2
like knock the flight attendants down in the back.
21:45:32.7
HOT-1
[sound of laughter]
21:45:34.5
HOT-2
like I'd see the flight attendants afterwards and they're like um who was
flying.
21:45:39.8
HOT-1
that would be that bonehead captain.
21:45:42.8
HOT-2
[sound of laughter]
21:45:44.0
HOT-1
you know what? yeah I tell you I'm getting a lot more used to it. uh I'm not
saying I like it any better but I am getting used to it.
21:45:51.0
HOT-2
yeah.
21:45:55.6
HOT-2
yeah I don't know what I want to do with the upgrade. I'm not entirely in
like a big rush to upgrade. um it would depend on where I'm based. just
because having to commute to be the bottom of the list is gonna suck.
and—.
21:46:07.0
HOT-1
true and— and you know like you were talking about as far as uh right
now your wanting to buy a house and wanting to have—.
21:46:13.6
HOT-2
exactly if I hold off— you know if it's a matter of holding on a few months
well then I'll be making a substantial amount more money in the— in the
Q than I would in the Saab.
21:46:22.0
HOT-1
right.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
251
21:46:22.9
HOT-2
depending you know how— how long would it be to make that worth my
while. would it— would I make more money upgrading into the Saab right
away or would I make more money if I waited for the Q for a little while.
21:46:32.6
HOT-1
well think of it this way uh if you— if you stayed on the on the Q obviously
you're gonna— you're not making the captain rate.
21:46:42.0
HOT-2
right.
21:46:42.5
HOT-1
but you may have a better quality of life to begin with uhh with regards to
buying a house and having a schedule to where you you know you could
work around and you could be—.
21:46:55.3
HOT-2
exactly.
21:46:55.6
HOT-1
you know home with your husband to to take care of all that kind of stuff.
21:46:59.6
HOT-2
exactly yeah it's just gonna depend where we're at when that happens.
but I— I mean I'm not— I'm not in such a hurry to upgrade. I've got very
very very good connections at Alaska.
21:47:10.4
HOT-1
oh cool.
21:47:11.2
HOT-2
Alaska's the only major I'd want to go to.
21:47:13.2
HOT-1
yeah.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
252
21:47:13.5
HOT-2
just because I don't want to commute my whole life...so um once I do
upgrade you know once once Alaska starts hiring I don't— I mean I don't
necessarily have to have a thousand hours PIC. I need to have some
PIC.
21:47:25.7
HOT-1
you don't have to with uh Alaska?
21:47:26.8
HOT-2
um it it depends. you you you do and on paper you do but it just— it it
depends who you know. if you know people then you can kind of sneak
away with it a little bit. I definitely need to have you know the proper
experience you need to be qualified. but if I have—.
21:47:36.6
HOT-1
huh...sure.
21:47:40.4
HOT-2
you know if at about five hundred hours they said to to go and interview
and then I can interview and they can say we want you to have a
thousand hours. so once you get a thousand hours um we're gonna put
you into ground school. they'll say stuff like that.
21:47:53.9
HOT-1
okay.
21:47:54.3
HOT-2
so I mean it depends and I don't even know if that's the route I want to go
anymore...you know the more I think about it. I wouldn't I wouldn't mind
flying for FedEx or UPS.
21:48:09.3
HOT-1
FedEx is still big on military time and the uh and the internal
recommendations so those two things— I mean that knocks me out of
FedEx for sure.
21:48:10.5
HOT-2
yeah...yeah.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
253
21:48:18.0
HOT-1
but uh UPS like I said I got my cousin that uh flies seven fives seven six.
he's based in Ontario.
21:48:26.3
HOT-2
yeah.
21:48:27.2
HOT-1
uh not too far from where he lives. but uh.
21:48:36.3
HOT-2
yeah I wouldn't mind— you know I could even see myself doing like I
mean for quality of life I could see myself doing cargo stuff and just I
mean like small stuff like there's a company that flies right out of my
hometown to Spokane Washington and back every night.
21:48:36.7
HOT-1
that's just—.
21:48:49.5
HOT
[tones similar to ACARS message reception]
21:48:51.2
HOT-2
and I'd do that three nights a week and be home. I could have kids and
raise a family. and I think that that might be more worth my while.
something like that.
21:48:58.5
HOT-1
yeah yeah.
21:48:59.6
HOT-2
and it just depends. I don't even know. I'm I'm so in limbo right now it's
actually kind of kind of interesting. like I don't know where I'll be in a year.
I don't know where I'll be in—.
21:49:05.4
HOT-1
well just keep your eyes open you know and and keep you know keep
listening uhh and and something will come across er you know you'll
know whenever it's time.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
254
21:49:18.2
HOT-2
yeah.
21:49:18.3
HOT-1
I've gotta do this. I've gotta— I'm ready to move on. um [sound similar to
yawn] excuse me. it's kind of like me. you know I started this this little gig
late in life.
21:49:28.7
HOT-2
yeah.
21:49:28.9
HOT-1
oh it's like it's a second career for me basically because I— I was able to
take that package with Verizon.
21:49:34.1
HOT-2
yeah.
21:49:35.5
HOT-1
but uh...you know it's...you know do I— g— at this point do I go to a major
and you know not be able to be there for very long.
21:49:48.8
HOT-2
yeah be an FO the rest of your life or...
21:49:51.8
HOT-1
uhh which— that may not be a bad thing as long as I would be able to
progress and and uh and be a lifetime FO if you will.
21:50:02.9
HOT-2
yeah yeah.
21:50:03.4
HOT-1
uh and just and and dwell upon the quality of life part of it or do I stay here
with Colgan and uh...
21:50:11.8
HOT-2
[sound of sneeze] excuse me.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
255
21:50:15.2
HOT-1
and you know likewise do the quality of life. I don't have to make two
hundred thousand dollars a year er a hundred fifty thousand dollars a
year whatever you know I could—.
21:50:20.7
HOT-2
exactly.
21:50:23.8
HOT-1
I can certainly be comfortable on on a hundred thousand. um you got
traffic out there just it's crossing left to right.
21:50:32.9
HOT-2
uh in sight.
21:50:35.4
HOT-1
but uh—.
21:50:41.8
HOT-2
um winds are at two fifty at fifteen gusting twenty three they're using
runway—.
21:50:45.0
ZNY-C
Colgan three four zero seven contact Cleveland Center one two
four point three two.
21:50:48.8
RDO-2
one two four point three two Colgan three four zero seven.
21:50:53.1
HOT-2
one two four thirty two.
21:50:58.5
RDO-2
Cleveland Center Colgan thirty four zero seven sixteen thousand.
21:51:02.1
ZOB
Colgan thirty four zero seven Cleveland Center roger.
21:51:05.4
HOT-2
alright so it's the winds are at two five zero fifteen gusting twenty three
and they're using three two and two three. do you want to use uh—.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
256
21:51:11.7
HOT-1
uh two three.
21:51:12.5
HOT-2
two three.
21:51:13.2
HOT-1
yeah.
21:51:13.7
HOT-2
okay.
21:51:13.8
HOT-?
[sound of sniffle]
21:51:16.3
HOT-1
and flaps fifteen.
21:51:18.3
HOT-2
okay.
21:51:21.7
HOT-2
uh it's runway two three.
21:51:23.8
HOT-1
ouch.
21:51:26.1
ZOB
Southwest six fifteen cleared direct to the Buffalo airport.
21:51:35.8
HOT-2
that us?
21:51:37.0
HOT-1
nope.
21:51:37.4
HOT-2
I didn't think so.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
257
21:51:38.6
HOT-1
yeah.
21:51:39.1
HOT-2
[sound of laughter] I just heard direct Buffalo.
21:51:42.0
HOT-2
uh does this look good to you? um...we've got TRAVA ILS two three
TRAVA KLUMP runway two three.
21:51:43.3
HOT-?
[sound of sniffle]
21:51:50.7
HOT-1
yeah TRAVA.
21:51:51.9
HOT-2
yeah here you go. and the EOA is in there.
21:51:53.0
HOT-?
[sound of sniffle]
21:51:59.4
HOT-1
thirty three.
21:52:03.7
HOT-?
[sound of sniffle]
21:52:05.1
HOT-1
try not to be dyslexic.
21:52:07.8
HOT-2
[sound of laughter]
21:52:08.2
HOT-1
last time I flew in here two thirty uh— two thirty three's the uh inbound
course. I put two twenty three.
21:52:14.2
HOT-2
oh geez. two thirty thirty three— no * it's runway— oh it is two thirty three?
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
258
21:52:19.6
HOT-1
it's two thirty three.
21:52:21.3
HOT-2
runway two three. oh yeah no that makes sense. now you got me
confused.
21:52:26.2
HOT-1
well I— well I didn't mean to confuse you now. two three three.
21:52:29.9
HOT-2
two three three.
21:52:31.0
HOT-1
and I'll brief it that way too.
21:52:32.6
HOT-2
alright it's two three three. [sound of laughter] we're good.
21:52:34.2
HOT-1
that's two three three.
21:52:53.2
HOT-?
[sound of sniffle]
21:52:57.2
HOT-2
alrighty and for the rest of that weather uh three miles. it's snowing with
some mist.
21:53:03.5
HOT-1
alright.
21:53:05.7
HOT-2
it didn't give me an RVR.
21:53:07.5
HOT-1
good...it's good.
21:53:10.9
HOT-2
that means it's far enough right?
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
259
21:53:13.9
HOT-1
yeah.
21:53:20.3
HOT-2
runway five then what do we have? one two nine two five.
21:53:30.4
HOT-?
[sound of sniffle]
21:53:40.2
HOT-2
alrighty your numbers. for flaps fifteen runway two three are eighteen and
fourteen.
21:53:43.1
HOT-?
[sound of sniffle]
21:53:47.5
HOT-1
alrighty eighteen and fourteen.
21:53:49.7
HOT-2
we have to go around it's gonna be twenty five and forty five.
21:54:05.5
HOT-?
[sound of sniffle]
21:54:06.7
HOT-2
alrighty. I don't think we had any specials did we?
21:54:12.0
HOT-1
uh I don't believe we did.
21:54:13.6
HOT
[sound of double chime]
21:54:16.9
INT-3
hello.
21:54:17.2
INT-2
hey any specials?
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
260
21:54:18.6
INT-3
uh no we don't.
21:54:19.8
INT-2
no specials.
21:54:20.6
INT-3
nope.
21:54:20.8
INT-2
we should be there in about twenty twenty five minutes.
21:54:23.0
INT-3
fantastic.
21:54:23.9
INT-2
alright
21:54:24.1
INT-3
thanks bye.
21:54:58.5
HOT-2
yeah I kind of like that I'm so flexible with what I'm doing.
21:55:01.3
CAM
[sound similar to seat track movement]
21:55:03.0
HOT-2
* I have goals but I have such a wide range of goals I don't know exactly
what I want.
21:55:05.3
HOT
[sound similar to double chime]
21:55:25.0
ZOB
Colgan thirty four zero seven Cleveland.
21:55:28.1
RDO-2
thirty four zero seven go ahead.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
261
21:55:30.2
ZOB
Colgan thirty four zero seven reset your transponder. squawk
seven— er uh two seven six two.
21:55:35.6
RDO-2
two seven six two Colgan thirty two— thirty four zero seven.
21:55:39.9
HOT-2
oops I think I had two seven six two I think I put half and half. two seven
six two yeah. twenty five and then I switched that one. oops.
21:55:56.8
HOT-?
[sound of sniffle]
21:56:08.0
HOT-1
it's just like we're in I don't know just just a light haze or type cloud. I don't
know just we can see things out in front of us.
21:56:17.4
HOT-2
do you want to go down?
21:56:18.6
HOT-1
huh? ohh. I was thinking about that.
21:56:26.4
HOT-2
might be easier on my ears if we start going down sooner.
21:56:28.9
HOT-1
yeah we could do it. that's fine.
21:56:31.6
RDO-2
and Center Colgan thirty four zero seven.
21:56:35.6
ZOB
Colgan thirty four zero seven uh say again?
21:56:35.9
HOT-1
get discretion to twelve.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
262
21:56:38.7
RDO-2
oh yeah just can we get PD down to twelve thousand for Colgan
thirty four zero seven.
21:56:42.6
ZOB
uhh standby.
21:56:44.9
HOT-1
I got your standby.
21:56:46.5
HOT-2
[sound of laughter]
21:56:49.5
HOT-?
[sound of sniffle]
21:57:07.1
HOT-1
we may have to wait for separation on this guy over here.
21:57:10.0
HOT-2
yeah.
21:57:10.8
ZOB
Colgan thirty four zero seven cross BENEE at maintain one one
thousand.
21:57:15.7
RDO-2
BENEE at one one eleven thousand Colgan thirty four zero seven.
21:57:20.5
HOT-2
BENEE at eleven.
21:57:21.3
HOT-1
tooo what was it?
21:57:23.2
HOT-2
BENEE.
21:57:23.4
HOT-1
oh BENEE.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
263
21:57:25.4
HOT-1
BENEE at one one thousand.
21:57:27.2
HOT-2
yes sir.
21:57:34.9
HOT-1
yeah that works.
21:58:28.0
HOT-?
[sound of sniffle]
21:58:31.1
HOT-1
you know we had a a controller down in Houston. uh he was known as
Mister Happy.
21:58:37.7
HOT-2
oh yeah.
21:58:38.4
HOT-1
guy was just he was— had a perfect personality for the being a controller.
he never let anything rattle him. and he just all just all bubbly type a type a
guy. he retired— just to let you know how he— how well respected he
was um he retired and he had they published where his retirement party
was. there was pilots from Continental Colgan pilots Chautauqua
Expressjet you know the main carriers there in Houston.
21:58:56.8
HOT-?
[sound of sniffles]
21:59:09.2
HOT-2
oh that's cool.
21:59:12.3
HOT-1
they all went to go see you know Mister Happy and everything but but
that's where I got the bent wing pencil jet.
21:59:19.6
HOT-2
it's where what?
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
264
21:59:20.6
HOT-1
that's where I got the bent wing pencil jet uh name from.
21:59:24.7
HOT-2
he calls them that?
21:59:26.4
HOT-1
yeah it was uh Jet Lincoln instead of Jetlink. called em Jet Lincoln and we
were Cold One.
21:59:29.0
HOT-2
uh-huh...oh.
21:59:32.4
HOT-1
Cold One nintey five sixty five you'll be following a bent wing pencil jet at
your one oh clock. two miles or whatever it was.
21:59:40.9
HOT-2
that's funny.
21:59:42.1
HOT-1
either that or you're following the lawn dart today. let's see uh if it was a
CRJ we're following the Barbie Jet.
21:59:45.6
HOT-2
[sound of laughter]
21:59:52.2
HOT-2
the Barbie Jet.
21:59:59.5
HOT-1
or he would say you're following Chi-tak-wa.
22:00:03.3
HOT-1
[sound of laughter]
22:00:04.1
HOT-2
[sound of laughter]
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
265
22:00:05.9
HOT-2
the guys that have fun and enjoy their jobs are so much more pleasant to
work with.
22:00:09.4
HOT-1
oh yeah.
22:00:10.8
HOT-2
yeah.
22:00:14.6
HOT-?
[sound of sniffle]
22:00:16.2
HOT-1
College Station Texas was a a contract control tower.
22:00:23.0
HOT-2
yeah.
22:00:23.2
HOT-1
had a guy that worked in there. had an odd accent to begin with. and uh
College Station Airport is uh owned and operated by the university— uh
the Texas A and M university.
22:00:37.8
ZOB
Mesaba thirty forty five contact Cleveland Center one two zero
point six.
22:00:39.7
HOT-2
uh-huh.
22:00:43.2
RDO-2
one two zero point six Colgan thirty four zero seven.
22:00:46.2
ZOB
nope Colgan thirty four zero seven you stay here. that was for
Mesaba.
22:00:49.8
HOT-2
oh.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
266
22:00:51.7
HOT-2
I'm not doing very good by * tonight.
22:00:52.7
HOT-1
it's alright.
22:00:54.0
ZOB
Colgan thirty four zero seven you still here?
22:00:56.3
RDO-2
yes sir thirty four zero seven.
22:00:59.5
HOT-1
sorry about that. oh anyway he would say Eeeeeeeeastwood information
echo.
22:01:08.9
HOT-2
[sound of laughter]
22:01:11.3
HOT-1
and he'd give us he'd give us same type of uh clearance to Houston.
Colgan ninety five twenty six you're cleared to the George Herbert Walker
er yeah George Herbert Walker Bush Intergalactical Airport.
22:01:27.6
HOT-2
[sound of laughter]
22:01:28.1
HOT-1
instead of Intercontinental. Intergalactical Airport via the College Station
zero seven six. baaaseball Rice won. climb maintain seven thousand.
departure frequency is Houston Center one two three point seven.
squawk whatever you know.
22:01:36.8
HOT-2
[sound of laughter]
22:01:47.6
HOT-2
yeah.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
267
22:01:48.0
HOT-1
and I would try to read it back exactly the same way. went in there I don't
know you know about three or four months before I left and he was just all
calm and quiet. you know I could tell it was him said hey man what
happened to that Eeeeeeastwood Airport information echo. he said yeah
they clipped my wings.
22:02:09.7
HOT-2
oh no. they didn't like him doing that?
22:02:12.3
HOT-1
I said well uh if if you need uh if you need any help on that one you just let
me know who to call and I'll uh be glad to put in a good word for ya. and
he he chuckled. he said uh he said awww let it blow over for a little while
and I'll be back I'll be back to my regular self later.
22:02:32.1
HOT-2
[sound of laughter]
22:02:32.9
HOT-1
yeah.
22:02:36.4
HOT-1
I just like the flying down there a whole lot better.
22:02:39.1
HOT-2
yeah.
22:02:39.6
HOT-1
see and and in the Saab in the northeast uh you * there's no FMS there's
no glass.
22:02:46.9
HOT-2
yeah.
22:02:47.5
HOT-1
and you're you're asses and elbows all the time.
22:02:51.5
HOT-2
yeah.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
268
22:02:52.4
HOT-1
uh because uh you're flying the the victor airways. the uh the VORs are
so close together and you're having to go to intersections.
22:03:00.3
HOT-2
yeah.
22:03:00.7
HOT-1
cross radials and all that kind of stuff. and uh it's it's hard work.
22:03:04.8
HOT-2
yeah.
22:03:05.3
HOT-1
down in Houston y— you're more spread out. uh the flying is a whole lot
nicer down there the controllers are a whole lot nicer. in Florida the same
way.
22:03:18.6
HOT-2
yeah Phoenix is like that.
22:03:20.3
HOT-?
[sound of sniffle]
22:03:21.2
HOT-1
man I— it's just all the pressure of all the the congestion and the the
volume and weather and anything and everything. the the controllers uh
they just it's like they uh constantly have their—.
22:03:38.1
ZOB
Colgan thirty four zero seven contact Buffalo Approach one two six
point one five.
22:03:41.8
HOT
[sound similar to altitude alert]
22:03:42.7
RDO-2
one two six one five Colgan thirty four zero seven.
22:03:45.4
HOT-1
twelve eleven alt sel.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
269
22:03:46.5
HOT-2
twelve eleven alt sel.
22:03:50.0
HOT-?
[sound of sniffle]
22:03:53.0
RDO-2
Buffalo Approach Colgan thirty four zero seven twelve for eleven
thousand with romeo.
22:03:59.2
APP
Colgan forty four zero seven Buff Approach good evening. Buffalo
altimeter's two niner eight zero. plan ILS approach runway two
three.
22:04:05.1
RDO-2
two niner eight zero and ILS two three Colgan thirty four zero
seven.
22:04:09.1
HOT-2
*.
22:04:09.3
HOT-1
two niner eight zero.
22:04:11.6
HOT-2
eight.
22:04:12.4
HOT-1
and we'll expect two three.
22:04:15.1
HOT-2
yup.
22:04:15.5
HOT-1
and if you've got your charts handy I'll brief it real quick.
22:04:17.7
HOT-2
IIII do.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
270
22:04:19.4
HOT-1
**. alright it's uh gonna be the ILS to uh runway two three at Buffalo. chart
eleven two twenty April oh seven.
22:04:28.9
HOT-2
yes sir.
22:04:29.7
HOT-1
got uh eleven three's the frequency set both sides. two thirty three set on
my side I saw you set yours. uh glideslope uh final approach fix uh
glideslope intercept is at the—.
22:04:39.9
APP
Colgan thirty four zero seven proceed direct TRAVA.
22:04:43.2
RDO-2
direct TRAVA Colgan thirty four zero seven.
22:04:45.8
HOT-2
direct—.
22:04:46.2
HOT-1
direct TRAVA.
22:04:50.6
HOT-1
oooh let's see I forget. do I do the do the first one?
22:04:54.8
HOT-2
I did the first one. it doesn't matter you could do either one. there's no
hold in there so—.
22:05:00.6
APP
Colgan thirty four zero seven descend and maintain six thousand.
22:05:03.8
RDO-2
sorry about that down to six thousand Colgan thirty four zero
seven.
22:05:08.2
HOT-2
cranky old guy.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
271
22:05:08.9
HOT-1
six thousand alt sel. that's something I you in in the Saab whoever if the
autopilot's engaged you know the pilot flying manipulates that #.
22:05:17.0
HOT-2
yeah...oh yeah.
22:05:20.7
HOT-1
I don't know why we don't do that here but we don't.
22:05:23.2
HOT-2
yeah.
22:05:24.3
HOT-1
alright well if you don't mind I'm gonna go ahead and push her on down at
a thousand feet a minute.
22:05:27.0
HOT-2
oh that's okay.
22:05:29.5
HOT-1
uh continuing on glideslope intercept's the outer marker twenty two oh six
that's fourteen uh seventy eight above the ground. DA's nine twenty eight
we'll put nine thirty in...it's also two hundred above the ground. touchdown
zone elevation is seven twenty eight. highest MSA's south of the outer
marker at thirty nine hundred north of the marker is twenty seven. and
ALSF two lighting uh missed approach is up to twenty three hundred
climbing right turn to three thousand via three hundred heading uh on the
uh two six seven radial to BUF VOR. and er outbound on VOR out to
WELLA uh which is DME twenty three point one uh hold uh this thing'll
probably do a parallel entry. uh we got the weather. bugs are set eighteen
fourteen flaps fifteen. uh off of twenty three I forget let me look it up.
22:06:05.0
HOT-?
[sound of sniffles]
22:06:31.0
HOT-2
left.
22:06:32.6
HOT-1
oh sure. I'll do it left turn.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
272
22:06:36.9
HOT-2
left turn.
22:06:37.6
HOT-1
first available.
22:06:38.7
HOT-2
I think so.
22:06:39.9
HOT-1
can I make echo?
22:06:41.3
HOT-2
um I think so.
22:06:42.9
HOT-1
okay.
22:06:45.3
HOT-1
we'll do it. oh #.
22:06:48.7
HOT-2
[sound of laughter]
22:06:50.5
HOT-1
going too far off.
22:06:55.6
HOT-2
yeah you can make echo.
22:06:55.8
HOT-1
*.
22:07:14.2
HOT-2
[sound similar to yawn] alright I'm gonna call in range. I'll be off one for a
second.
22:07:16.8
HOT-1
I got one.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
273
22:07:18.3
HOT-2
* two five right? yup.
22:07:21.2
HOT-?
[sound of sniffle]
22:07:22.1
RDO-2
Ops Colgan thirty four zero seven's in range.
22:07:29.9
HOT-?
[sound of sniffle]
22:07:30.6
OPS
thirty four zero seven go for Buffalo ops.
22:07:33.4
RDO-2
yeah we're just letting you know we're in range. uh let's see here
looks like we're ten maybe fifteen minutes out.
22:07:39.2
OPS
we'll see you in about ten fifteen minutes. gate twenty six. um we
do actually have another Colgan turn we're trying to get out uh
because they have the adapter we need to meet you guys. um so it
might be just a couple minutes when you get here before we can
actually bring the jetbridge up to ya.
22:07:54.2
RDO-2
alrighty uh thirty four zero seven we'll be we'll be ready for that
thanks.
22:07:58.6
OPS
thank you see you then.
22:07:59.9
HOT-1
is the other Colgan in?
22:08:02.3
HOT-2
the other Colgan's there right now. and they're trying to turn him and we
may have to sit and wait for them to turn him.

NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
274
22:08:07.4
HOT-1
yeah.
22:08:08.4
HOT-2
that's what she said.
22:08:09.1
HOT-1
how'd they beat us?
22:08:11.8
HOT-2
I don't— they must have taken runway two niner. 'cause they— we we sat
there for like forty five minutes without anybody taking off two two.
22:08:26.4
HOT-?
[sound of sniffle]
22:08:27.5
HOT-1
alrighty.
22:08:37.4
HOT-?
[sound of sniffle]
22:08:41.0
HOT-2
alrighty **.
22:08:41.4
APP
Colgan thirty four zero seven descend and maintain five thousand.
22:08:45.0
RDO-2
five thousand Colgan thirty four zero seven.
22:08:47.9
HOT-1
five thousand alt sel.
22:08:48.9
HOT-2
five thousand alt sel I'm off one.
22:08:50.2
HOT-1
I've got one.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
275
22:08:51.1
PA-2
folks from the flight deck your first officer speaking uh it looks like at this
time we're about ten maybe fifteen minutes outside of Buffalo. weather in
Buffalo is uh pretty foggy. uh snowing a little bit there it's not too terribly
cold uh but uh at this time I'd like to make sure everybody remains in their
seats so the flight attendants can prepare the cabin for arrival. thank you.
22:09:10.6
HOT-2
[sound of sniffles] alrighty I'm back on one.
22:09:12.1
APP
Colgan thirty four zero seven descend and maintain four thousand.
22:09:15.6
RDO-2
and four thousand Colgan thirty four zero seven.
22:09:15.9
PA-3
ladies and gentlemen in preparation for landing in Buffalo please be
certain your seatback is straight up and your seatbelt is fastened. please
pass any remaining service items and unwanted reading materials to us
as we pass through the cabin. please turn off all portable electronic
devices and stow them until we have reached the gate. after landing
Continental Connection allows passengers to use cell phones. I will make
an announcement when it is safe to use this device. if you plan to use
your cell phone please ensure it's accessible since personal items must
be stowed until we reach the gate.
22:09:17.8
HOT-1
four thousand alt sel.
22:09:18.8
HOT-2
four thousand.
22:09:26.0
HOT-1
how's the ears?
22:09:27.3
HOT-2
uh they're stuffy.
22:09:31.6
HOT-1
are they poppin?
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
276
22:09:32.7
HOT-2
yeah.
22:09:33.3
HOT-1
okay. that's a good thing.
22:09:35.7
HOT-2
yeah I wanna make em pop. [sound of laughter]
22:10:20.6
HOT-?
[sound of sniffle]
22:10:22.6
HOT-2
is that ice on our windshield?
22:10:25.6
HOT-1
got it on my side. you don't have yours?
22:10:28.7
HOT-1
* [sound of whistle]
22:10:29.2
HOT-?
[sound of sniffle]
22:10:30.5
CAM
[sound of click]
22:10:32.3
HOT-2
oh yeah oh it's lots of ice.
22:10:39.5
HOT-?
[sound of sniffle]
22:10:47.5
HOT-1
oh yeah that's the most I've seen— most ice I've seen on the leading
edges in a long time. in a while anyway I should say.
22:10:51.4
HOT-2
oh *.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
277
22:10:56.8
HOT-?
[sound of sniffle]
22:10:57.7
HOT-2
yeah that's another thing. all the guys— @ came in to our when we
interviewed and he said oh yeah you'll all be upgraded in six months into
the Saab and blah ba blah ba blah and I'm thinking you know what. flying
in the northeast I've sixteen hundred hours. all of that in Phoenix how
much time do you think actual I had or any in in ice. I had more actual
time on my first day of IOE than I did in the sixteen hundred hours I had
when I came here.
22:11:14.8
HOT-?
[sound of sniffle]
22:11:21.0
HOT-1
[sound of laughter]
22:11:22.2
HOT-2
I'm not even kidding. the first day.
22:11:25.7
HOT-1
well that sounds— well I mean I didn't have sixteen hundred hours.
22:11:27.5
HOT
[sound similar to altitude alert]
22:11:28.9
HOT-1
five for four alt sel.
22:11:29.8
HOT-2
five four alt sel.
22:11:31.1
HOT-?
[sound of sniffle]
22:11:31.5
HOT-1
but uh as a matter of fact I got hired with about six hundred and twenty
five hours here.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
278
22:11:37.6
HOT-2
oh wow.
22:11:39.4
HOT-1
uh.
22:11:39.9
HOT-2
that's not much for uh back when you got hired.
22:11:42.5
HOT-1
no but uh out of that six and a quarter two hundred fifty hours was uh part
one twenty one turbine. multi engine turbine.
22:11:50.0
HOT-2
oh that's right yeah.
22:11:54.3
HOT-2
no but all these guys are complaining they're saying you know how we
were supposed to upgrade by now and they're complaining I'm thinking
you know what? I really wouldn't mind going through a a winter in the
northeast before I have to upgrade to captain.
22:12:04.0
HOT-1
no no.
22:12:05.0
HOT-2
I've never seen icing conditions. I've never deiced. I've never seen any—
I've never experienced any of that. I don't want to have to experience that
and make those kinds of calls. you know I'dve freaked out. I'dve have like
seen this much ice and thought oh my gosh we were going to crash.
22:12:17.7
APP
Colgan thirty four oh seven descend and maintain two thousand
three hundred.
22:12:21.8
RDO-2
okay down to two thousand three hundred Colgan thirty four zero
seven.
22:12:25.1
HOT-2
um two three alt sel.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
279
22:12:27.4
HOT-2
I've got you in pitch pitch hold. I don't know if that's what you want.
22:12:27.6
HOT-1
two three alt sel.
22:12:29.6
HOT-1
yeah that's alright. let's uh— we'll do vertical speed back.
22:12:33.3
HOT-2
but I'm glad to have seen oh— you know now I'm so much more
comfortable with it all.
22:12:37.6
HOT-1
yeah uh I I spent the first three months in uh Charleston West Virginia and
uh flew—.
22:12:43.5
APP
Colgan thirty four zero seven turn left heading three three zero.
22:12:47.0
RDO-2
left heading three three zero Colgan thirty four zero seven.
22:12:49.3
HOT-1
left three three zerooo. we're in heading mode now. go to blue needles.
22:13:01.2
HOT-1
but I— first couple of times I saw the amount of ice that that Saab would
would pick up and keep on truckin'.
22:13:05.9
HOT-2
yeah.
22:13:06.7
HOT-?
[sound of sniffle]
22:13:08.0
HOT-1
saw it out on the spinner. ice comin' out about that far my eyes about that
big around. I'm going gosh. I mean Florida man— barely a little you know
out of Pensacola.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
280
22:13:09.3
HOT-2
yeah.
22:13:14.2
HOT-2
holy cow...oh my gosh...oh yeah.
22:13:18.0
HOT
[sound similar to altitude alert]
22:13:21.4
HOT-1
that's uh thirty three for twenty three alt sel.
22:13:24.1
HOT-2
thirty three for twenty three alt sel.
22:13:24.8
HOT-1
let's do a descent checklist please.
22:13:25.9
HOT-2
do a descent checklist. altimeters two niner eight zero set crosschecked.
22:13:29.1
HOT-1
twenty nine eighty set crosschecked.
22:13:30.8
HOT-2
fuel balance check. pressurization set and cabin PA complete. descent
checklist complete.
22:13:35.7
HOT-1
alright if you want to go ahead we can do the approach checklist along
with it.
22:13:37.4
HOT-2
yeah sure. um approach checklist approach and landing brief complete.
22:13:41.6
HOT-1
uh complete.
22:13:42.3
HOT-2
bugs set.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
281
22:13:43.3
HOT-1
set.
22:13:44.3
HOT-2
GPWS landing flaps selected fifteen degrees. fuel transfer off hydraulic
pressure and quantity check. caution warning lights check seatbelt sign
on and external lights on. approach checklist complete.
22:13:54.5
HOT-2
[sound of sniffle]
22:13:54.7
HOT-1
rock and roll.
22:13:58.4
HOT-2
oh yeah— I'm so glad. I would've— I w— I mean—. I would've been been
fine. I would have survived it. there wasn't— we n— never had to make
decisions that I wouldn't have been able to make but...now I'm more
comfortable.
22:14:08.5
APP
Colgan thirty four zero seven turn left heading three one zero.
22:14:12.1
RDO-2
left heading three one zero for Colgan thirty four zero seven.
22:14:12.7
CAM
[sound similar to engine power increase]
22:14:14.6
HOT-1
three one zero.
22:14:16.6
HOT-2
yeah.
22:14:21.9
HOT-?
[sound of sniffles]
22:14:22.6
HOT-1
alright let's see if I can get this seat...siteated...that's alright there.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
282
22:14:24.7
CAM
[sound similar to seat track movement]
22:14:32.7
HOT-1
still trying to find that sweet spot I guess there *.
22:14:39.8
CAM
[sound similar to engine power increase]
22:14:56.7
HOT-?
[sound of sniffle]
22:15:06.3
HOT-1
flaps five. [covered by background radio transmissions]
22:15:08.1
HOT-2
what?
22:15:08.8
HOT-1
flaps five please.
22:15:10.0
HOT-2
oh *.
22:15:11.2
CAM
[sound similar to flap handle movement]
22:15:13.2
HOT-?
[sound of sniffle]
22:15:13.5
APP
Colgan thirty four zero seven three miles from KLUMP turn left
heading two six zero maintain two thousand three hundred until
established localizer. cleared ILS approach runway two three.
22:15:22.2
RDO-2
left two sixty two thousand three hundred 'til established and
cleared ILS two three approach Colgan thirty four zero seven.
22:15:31.7
HOT-1
alright approach is armed.
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
283
22:15:32.8
HOT-2
roger.
22:15:38.8
HOT-?
[sound of sniffle]
22:15:59.5
CAM
[sound similar to decrease in engine power]
22:16:04.1
HOT-1
gear down...loc's alive.
22:16:06.2
CAM
[sound similar to landing gear handle movement]
22:16:06.4
APP
Colgan thirty four zero seven contact tower one two zero point five.
have a good night.
22:16:07.4
CAM
[sound similar to landing gear deployment]
22:16:11.5
RDO-2
over to tower you do the same thirty four zero seven.
22:16:14.9
HOT
[sound of two double chimes]
22:16:19.2
HOT-?
[sound of sniffle]
22:16:21.2
HOT-2
gear's down.
22:16:23.5
HOT-1
flaps fifteen before landing checklist.
22:16:26.0
CAM
[sound similar to flap handle movement]
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
284
22:16:26.6
HOT-2
uhhh.
22:16:27.4
CAM
[sound similar to stick shaker lasting 6.7 seconds]
22:16:27.7
HOT
[sound similar to autopilot disconnect horn repeats until end of recording]
22:16:27.9
CAM
[sound of click]
22:16:31.1
CAM
[sound similar to increase in engine power]
22:16:34.8
HOT-1
Jesus Christ.
22:16:35.4
CAM
[sound similar to stick shaker lasting until end of recording]
22:16:37.1
HOT-2
I put the flaps up.
22:16:40.2
CAM
[sound of two clicks]
22:16:42.2
HOT-1
[sound of grunt] *ther bear.
22:16:45.8
HOT-2
should the gear up?
22:16:46.8
HOT-1
gear up oh #.
22:16:50.1
CAM
[increase in ambient noise]
NTSB Aircraft Accident Report
INTRA-AIRCRAFT COMMUNICATION AIR-GROUND COMMUNICATION
TIME and TIME and
SOURCE CONTENT SOURCE CONTENT
285
22:16:51.9
HOT-1
we're down.
22:16:51.9
CAM
[sound of thump]
22:16:52.0
HOT-2
we're [sound of scream]
22:16:53.9
END OF TRANSCRIPT
END OF RECORDING
